
Page 260 - Textbook of Pathology, 6th Edition
P. 260
244 for age, sex and height is considered a health risk. The most widely
used method to gauge obesity is body mass index (BMI)
2
which is equal to weight in kg/height in m . A cut off BMI
value of 30 is used for obesity in both men and women.
ETIOLOGY. Obesity results when caloric intake exceeds utili-
sation. The imbalance of these two components can occur in
the following situations:
1. Inadequate pushing of oneself away from the dining table
SECTION I
causing overeating.
2. Insufficient pushing of oneself out of the chair leading to
inactivity and sedentary life style.
3. Genetic predisposition to develop obesity.
4. Diets largely derived from carbohydrates and fats than
protein-rich diet.
5. Secondary obesity may result following a number of under-
lying diseases such as hypothyroidism, Cushing’s disease,
insulinoma and hypothalamic disorders.
PATHOGENESIS. The lipid storing cells, adipocytes
comprise the adipose tissue, and are present in vascular and
stromal compartment in the body. Besides the generally
accepted role of adipocytes for fat storage, these cells also
release endocrine-regulating molecules. These molecules
include: energy regulatory hormone (leptin), cytokines
(TNF-α and interleukin-6), insulin sensitivity regulating
agents (adiponectin, resistin and RBP4), prothrombotic
factors (plasminogen activator inhibitor), and blood pressure
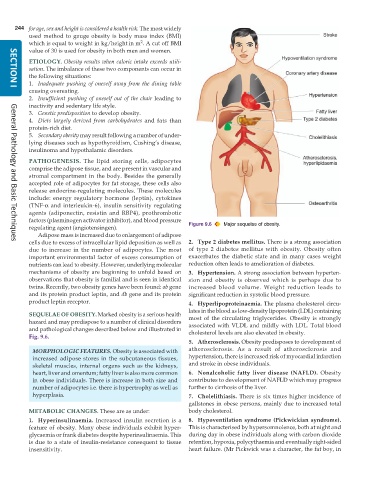
regulating agent (angiotensingen). Figure 9.6 Major sequelae of obesity.
Adipose mass is increased due to enlargement of adipose
cells due to excess of intracellular lipid deposition as well as 2. Type 2 diabetes mellitus. There is a strong association
General Pathology and Basic Techniques
due to increase in the number of adipocytes. The most of type 2 diabetes mellitus with obesity. Obesity often
important environmental factor of excess consumption of exacerbates the diabetic state and in many cases weight
nutrients can lead to obesity. However, underlying molecular reduction often leads to amelioration of diabetes.
mechanisms of obesity are beginning to unfold based on 3. Hypertension. A strong association between hyperten-
observations that obesity is familial and is seen in identical sion and obesity is observed which is perhaps due to
twins. Recently, two obesity genes have been found: ob gene increased blood volume. Weight reduction leads to
and its protein product leptin, and db gene and its protein significant reduction in systolic blood pressure.
product leptin receptor. 4. Hyperlipoproteinaemia. The plasma cholesterol circu-
lates in the blood as low-density lipoprotein (LDL) containing
SEQUELAE OF OBESITY. Marked obesity is a serious health most of the circulating triglycerides. Obesity is strongly
hazard and may predispose to a number of clinical disorders associated with VLDL and mildly with LDL. Total blood
and pathological changes described below and illustrated in cholesterol levels are also elevated in obesity.
Fig. 9.6.
5. Atherosclerosis. Obesity predisposes to development of
MORPHOLOGIC FEATURES. Obesity is associated with atherosclerosis. As a result of atherosclerosis and
increased adipose stores in the subcutaneous tissues, hypertension, there is increased risk of myocardial infarction
skeletal muscles, internal organs such as the kidneys, and stroke in obese individuals.
heart, liver and omentum; fatty liver is also more common 6. Nonalcoholic fatty liver disease (NAFLD). Obesity
in obese individuals. There is increase in both size and contributes to development of NAFLD which may progress
number of adipocytes i.e. there is hypertrophy as well as further to cirrhosis of the liver.
hyperplasia. 7. Cholelithiasis. There is six times higher incidence of
gallstones in obese persons, mainly due to increased total
METABOLIC CHANGES. These are as under: body cholesterol.
1. Hyperinsulinaemia. Increased insulin secretion is a 8. Hypoventilation syndrome (Pickwickian syndrome).
feature of obesity. Many obese individuals exhibit hyper- This is characterised by hypersomnolence, both at night and
glycaemia or frank diabetes despite hyperinsulinaemia. This during day in obese individuals along with carbon dioxide
is due to a state of insulin-resistance consequent to tissue retention, hypoxia, polycythaemia and eventually right-sided
insensitivity. heart failure. (Mr Pickwick was a character, the fat boy, in