
Page 542 - Textbook of Pathology, 6th Edition
P. 542
526
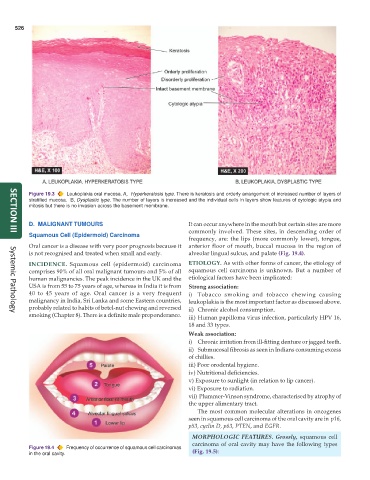
Figure 19.3 Leukoplakia oral mucosa. A, Hyperkeratosis type. There is keratosis and orderly arrangement of increased number of layers of
stratified mucosa. B, Dysplastic type. The number of layers is increased and the individual cells in layers show features of cytologic atypia and
mitosis but there is no invasion across the basement membrane.
D. MALIGNANT TUMOURS It can occur anywhere in the mouth but certain sites are more
commonly involved. These sites, in descending order of
Squamous Cell (Epidermoid) Carcinoma
SECTION III
frequency, are: the lips (more commonly lower), tongue,
Oral cancer is a disease with very poor prognosis because it anterior floor of mouth, buccal mucosa in the region of
is not recognised and treated when small and early. alveolar lingual sulcus, and palate (Fig. 19.4).
INCIDENCE. Squamous cell (epidermoid) carcinoma ETIOLOGY. As with other forms of cancer, the etiology of
comprises 90% of all oral malignant tumours and 5% of all squamous cell carcinoma is unknown. But a number of
human malignancies. The peak incidence in the UK and the etiological factors have been implicated:
USA is from 55 to 75 years of age, whereas in India it is from Strong association:
40 to 45 years of age. Oral cancer is a very frequent i) Tobacco smoking and tobacco chewing causing
malignancy in India, Sri Lanka and some Eastern countries, leukoplakia is the most important factor as discussed above.
probably related to habits of betel-nut chewing and reversed ii) Chronic alcohol consumption.
smoking (Chapter 8). There is a definite male preponderance. iii) Human papilloma virus infection, particularly HPV 16,
Systemic Pathology
18 and 33 types.
Weak association:
i) Chronic irritation from ill-fitting denture or jagged teeth.
ii) Submucosal fibrosis as seen in Indians consuming excess
of chillies.
iii) Poor orodental hygiene.
iv) Nutritional deficiencies.
v) Exposure to sunlight (in relation to lip cancer).
vi) Exposure to radiation.
vii) Plummer-Vinson syndrome, characterised by atrophy of
the upper alimentary tract.
The most common molecular alterations in oncogenes
seen in squamous cell carcinoma of the oral cavity are in p16,
p53, cyclin D, p63, PTEN, and EGFR.
MORPHOLOGIC FEATURES. Grossly, squamous cell
carcinoma of oral cavity may have the following types
Figure 19.4 Frequency of occurrence of squamous cell carcinomas (Fig. 19.5):
in the oral cavity.