
Page 572 - Textbook of Pathology, 6th Edition
P. 572
556
Figure 20.16 Classifications of gastric carcinomas. A, Conventional classification, showing correlation of the macroscopic subtypes with the
main histological patterns. B, Classification based on the depth of invasion by the tumour.
I. Expanding (formerly intestinal type) carcinomas that Prognosis of EGC after surgical resection is quite good;
grow laterally by an invasive margin. The tumour cells 5-year survival rate being 93-99%.
are in the form of cohesive clusters. Early gastric carcinoma must be distinguished from
II. Infiltrating (formerly diffuse type) carcinomas have certain related terms as under:
poorly-defined invasive border. The tumour cells are loose Epithelial dysplasia is cellular atypia seen in intestinal
and invade singly or in small group. metaplasia such as in atrophic gastritis and pernicious
These classifications are summarised in Fig. 20.16 and anaemia.
comparative morphology of various types is shown Carcinoma in situ in the stomach is a state of severe
diagrammatically in Fig. 20.18. cellular atypia or dysplasia, without invasion across the
I. EARLY GASTRIC CARCINOMA (EGC) (Fig. basement membrane of the glands.
20.18,A). EGC is the term used to describe cancer limited II. ADVANCED GASTRIC CARCINOMA. When the
to the mucosa and submucosa. The diagnosis of this carcinoma crosses the basement membrane into the
SECTION III
condition has been made possible by extensive work on muscularis propria or beyond, it is referred to as advanced
histogenesis of gastric cancer by Japanese pathologists by gastric carcinoma. Advanced gastric carcinoma has
the use of fibreoptic endoscope and gastrocamera. In following 5 patterns:
Japan, EGC comprises 35% of newly-diagnosed cases of i) Ulcerative carcinoma (Fig. 20.18,B). This is the most
gastric cancer. common pattern. The tumour appears as a flat, infiltrating
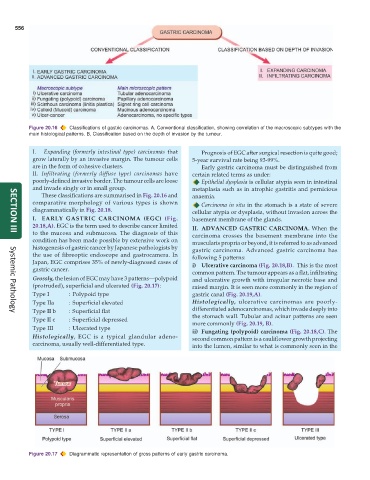
Grossly, the lesion of EGC may have 3 patterns—polypoid and ulcerative growth with irregular necrotic base and
(protruded), superficial and ulcerated (Fig. 20.17): raised margin. It is seen more commonly in the region of
Type I : Polypoid type gastric canal (Fig. 20.19,A).
Type IIa : Superficial elevated Histologically, ulcerative carcinomas are poorly-
Type II b : Superficial flat differentiated adenocarcinomas, which invade deeply into
Systemic Pathology
Type II c : Superficial depressed the stomach wall. Tubular and acinar patterns are seen
more commonly (Fig. 20.19, B).
Type III : Ulcerated type ii) Fungating (polypoid) carcinoma (Fig. 20.18,C). The
Histologically, EGC is a typical glandular adeno- second common pattern is a cauliflower growth projecting
carcinoma, usually well-differentiated type. into the lumen, similar to what is commonly seen in the
Figure 20.17 Diagrammatic representation of gross patterns of early gastric carcinoma.