
Page 613 - Textbook of Pathology, 6th Edition
P. 613
erythrocytes at the end of their normal lifespan of 120 days 597
takes place in the reticuloendothelial system in the bone
marrow, spleen and liver. The remaining 15-20% of the
bilirubin comes partly from non-haemoglobin haem-
containing pigments such as myoglobin, catalase and
cytochromes, and partly from ineffective erythropoiesis. In
either case, haem moiety is formed which is converted to
biliverdin by microsomal haem oxygenase for which oxygen
and NADPH are essential requirements. Bilirubin is formed
from biliverdin by biliverdin reductase.
2. TRANSPORT OF BILIRUBIN. Bilirubin on release from
macrophages circulates as unconjugated bilirubin in plasma
tightly bound to albumin. Certain drugs such as
sulfonamides and salicylates compete with bilirubin for
albumin binding and displace bilirubin from albumin, thus
facilitating bilirubin to enter into the brain in neonates and
increase the risk of kernicterus. Bilirubin is found in body
fluids in proportion to their albumin content such as in CSF,
joint effusions, cysts etc.
3. HEPATIC PHASE. On coming in contact with the
hepatocyte surface, unconjugated bilirubin is preferentially
metabolised which involves 3 steps: hepatic uptake,
conjugation and secretion in bile.
i) Hepatic uptake: Albumin-bound unconjugated bilirubin
upon entry into the hepatocyte, is dissociated into bilirubin CHAPTER 21
and albumin. The bilirubin gets bound to cytoplasmic protein
glutathione-S-transferase (GST) (earlier called ligandin).
ii) Conjugation: Unconjugated bilirubin is not water-soluble
but is alcohol-soluble and is converted into water-soluble
compound by conjugation. Conjugation occurs in
endoplasmic reticulum and involves conversion to bilirubin
mono- and diglucuronide by the action of microsomal
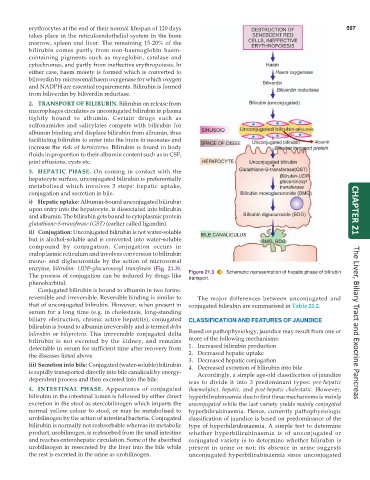
enzyme, bilirubin- UDP-glucuronosyl transferase (Fig. 21.3).
The process of conjugation can be induced by drugs like Figure 21.3 Schematic representation of hepatic phase of bilirubin
transport.
phenobarbital.
Conjugated bilirubin is bound to albumin in two forms:
reversible and irreversible. Reversible binding is similar to The major differences between unconjugated and
that of unconjugated bilirubin. However, when present in conjugated bilirubin are summarised in Table 21.2.
serum for a long time (e.g. in cholestasis, long-standing
biliary obstruction, chronic active hepatitis), conjugated CLASSIFICATION AND FEATURES OF JAUNDICE
bilirubin is bound to albumin irreversibly and is termed delta The Liver, Biliary Tract and Exocrine Pancreas
bilirubin or biliprotein. This irreversible conjugated delta Based on pathophysiology, jaundice may result from one or
bilirubin is not excreted by the kidney, and remains more of the following mechanisms:
detectable in serum for sufficient time after recovery from 1. Increased bilirubin production
the diseases listed above. 2. Decreased hepatic uptake
3. Decreased hepatic conjugation
iii) Secretion into bile: Conjugated (water-soluble) bilirubin 4. Decreased excretion of bilirubin into bile
is rapidly transported directly into bile canaliculi by energy- Accordingly, a simple age-old classification of jaundice
dependent process and then excreted into the bile.
was to divide it into 3 predominant types: pre-hepatic
4. INTESTINAL PHASE. Appearance of conjugated (haemolytic), hepatic, and post-hepatic cholestatic. However,
bilirubin in the intestinal lumen is followed by either direct hyperbilirubinaemia due to first three mechanisms is mainly
excretion in the stool as stercobilinogen which imparts the unconjugated while the last variety yields mainly conjugated
normal yellow colour to stool, or may be metabolised to hyperbilirubinaemia. Hence, currently pathophysiologic
urobilinogen by the action of intestinal bacteria. Conjugated classification of jaundice is based on predominance of the
bilirubin is normally not reabsorbable whereas its metabolic type of hyperbilirubinaemia. A simple test to determine
product, urobilinogen, is reabsorbed from the small intestine whether hyperbilirubinaemia is of unconjugated or
and reaches enterohepatic circulation. Some of the absorbed conjugated variety is to determine whether bilirubin is
urobilinogen in resecreted by the liver into the bile while present in urine or not; its absence in urine suggests
the rest is excreted in the urine as urobilinogen. unconjugated hyperbilirubinaemia since unconjugated