
Page 630 - Textbook of Pathology, 6th Edition
P. 630
614 3. Hepatitis D. Hepatitis D infection can also be prevented
by hepatitis B vaccine.
4. Hepatitis C. Currently, hepatitis C vaccine has yet not
been feasible though antibodies to HCV envelope have been
developed.
5. Hepatitis E. It is not certain whether immune globulin
(like for HAV) prevents hepatitis E infection or not but a
vaccine against HEV is yet to be developed.
OTHER INFECTIONS AND INFESTATIONS
Apart from viral hepatitis, the liver is affected by infections
with bacteria, spirochaetes and fungi and is involved in some
parasitic infestations. Some common examples of such
conditions are described below.
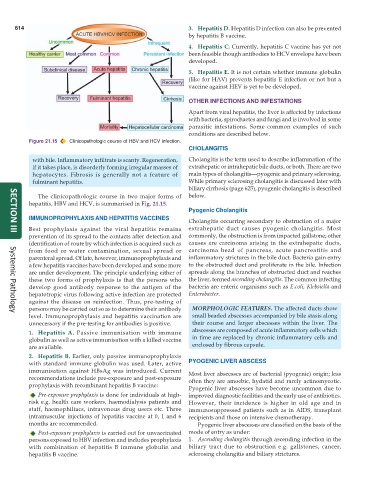
Figure 21.15 Clinicopathologic course of HBV and HCV infection.
CHOLANGITIS
with bile. Inflammatory infiltrate is scanty. Regeneration, Cholangitis is the term used to describe inflammation of the
if it takes place, is disorderly forming irregular masses of extrahepatic or intrahepatic bile ducts, or both. There are two
hepatocytes. Fibrosis is generally not a feature of main types of cholangitis—pyogenic and primary sclerosing.
fulminant hepatitis. While primary sclerosing cholangitis is discussed later with
biliary cirrhosis (page 625), pyogenic cholangitis is described
The clinicopathologic course in two major forms of below.
hepatitis, HBV and HCV, is summarised in Fig. 21.15.
Pyogenic Cholangitis
IMMUNOPROPHYLAXIS AND HEPATITIS VACCINES
Cholangitis occurring secondary to obstruction of a major
Best prophylaxis against the viral hepatitis remains extrahepatic duct causes pyogenic cholangitis. Most
prevention of its spread to the contacts after detection and commonly, the obstruction is from impacted gallstone; other
SECTION III
identification of route by which infection is acquired such as causes are carcinoma arising in the extrahepatic ducts,
from food or water contamination, sexual spread or carcinoma head of pancreas, acute pancreatitis and
parenteral spread. Of late, however, immunoprophylaxis and inflammatory strictures in the bile duct. Bacteria gain entry
a few hepatitis vaccines have been developed and some more to the obstructed duct and proliferate in the bile. Infection
are under development. The principle underlying either of spreads along the branches of obstructed duct and reaches
these two forms of prophylaxis is that the persons who the liver, termed ascending cholangitis. The common infecting
develop good antibody response to the antigen of the bacteria are enteric organisms such as E.coli, Klebsiella and
hepatotropic virus following active infection are protected Enterobacter.
against the disease on reinfection. Thus, pre-testing of
persons may be carried out so as to determine their antibody MORPHOLOGIC FEATURES. The affected ducts show
Systemic Pathology
level. Immunoprophylaxis and hepatitis vaccination are small beaded abscesses accompanied by bile stasis along
unnecessary if the pre-testing for antibodies is positive. their course and larger abscesses within the liver. The
1. Hepatitis A. Passive immunisation with immune abscesses are composed of acute inflammatory cells which
globulin as well as active immunisation with a killed vaccine in time are replaced by chronic inflammatory cells and
are available. enclosed by fibrous capsule.
2. Hepatitis B. Earlier, only passive immunoprophylaxis
with standard immune globulin was used. Later, active PYOGENIC LIVER ABSCESS
immunisation against HBsAg was introduced. Current Most liver abscesses are of bacterial (pyogenic) origin; less
recommendations include pre-exposure and post-exposure often they are amoebic, hydatid and rarely actinomycotic.
prophylaxis with recombinant hepatitis B vaccine:
Pyogenic liver abscesses have become uncommon due to
Pre-exposure prophylaxis is done for individuals at high- improved diagnostic facilities and the early use of antibiotics.
risk e.g. health care workers, haemodialysis patients and However, their incidence is higher in old age and in
staff, haemophiliacs, intravenous drug users etc. Three immunosuppressed patients such as in AIDS, transplant
intramuscular injections of hepatitis vaccine at 0, 1 and 6 recipients and those on intensive chemotherapy.
months are recommended. Pyogenic liver abscesses are classified on the basis of the
Post-exposure prophylaxis is carried out for unvaccinated mode of entry as under:
persons exposed to HBV infection and includes prophylaxis 1. Ascending cholangitis through ascending infection in the
with combination of hepatitis B immune globulin and biliary tract due to obstruction e.g. gallstones, cancer,
hepatitis B vaccine. sclerosing cholangitis and biliary strictures.