
Page 90 - AACN Essentials of Critical-Care Nursing Pocket Handbook, Second Edition
P. 90
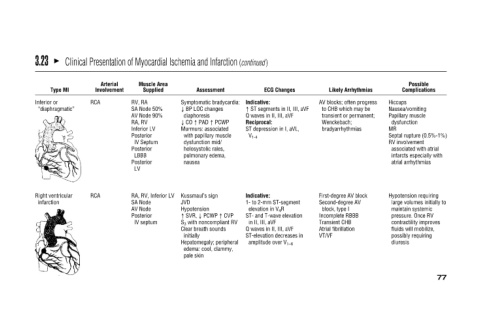
Possible Complications Septal rupture (0.5%-1%) associated with atrial infarcts especially with atrial arrhythmias Hypotension requiring large volumes initially to maintain systemic pressure. Once RV contractility improves fluids wi
Hiccups Nausea/vomiting Papillary muscle dysfunction MR RV involvement diuresis
Likely Arrhythmias AV blocks; often progress to CHB which may be transient or permanent; Wenckebach; bradyarrhythmias First-degree AV block Second-degree AV block, type I Incomplete RBBB Transient CHB Atrial fibrillation VT/VF
ECG Changes ↑ ST segments in II, III, aVF Q waves in II, III, aVF ST depression in I, aVL, 1- to 2-mm ST-segment ST- and T-wave elevation Q waves in II, III, aVF ST-elevation decreases in amplitude over V 1–6
Indicative: Reciprocal: V 1-4 Indicative: elevation in V 4 R in II, III, aVF
Clinical Presentation of Myocardial Ischemia and Infarction (continued)
Assessment Symptomatic bradycardia: ↓ BP LOC changes diaphoresis ↓ CO ↑ PAD ↑ PCWP Murmurs: associated with papillary muscle dysfunction mid/ holosystolic rales, pulmonary edema, nausea Kussmaul’s sign JVD Hypotension ↑ SVR, ↓
Muscle Area Supplied RV, RA SA Node 50% AV Node 90% RA, RV Inferior LV Posterior IV Septum Posterior LBBB Posterior LV RA, RV, Inferior LV SA Node AV Node Posterior IV septum
Arterial Involvement RCA RCA
Type MI
“diaphragmatic” Right ventricular
3.23 Inferior or infarction