
Page 212 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 212
8 Genetic and Paediatric Disorders 197
2. Autosomal recessive (AR) disorders
(a) Largest group of Mendelian disorders.
(b) Both abnormal alleles must be present (homozygous state) to express the
disease.
(c) The trait does not always affect the parents but siblings may be affected.
(d) The chance siblings getting affected is one in four.
(e) May result from a consanguineous marriage.
(f) The expression of the defect appears to be more uniform than in AD disorders.
(g) Complete penetrance is common.
(h) Onset is frequently early in life.
(i) Because the affected individual may be an asymptomatic heterozygote, new
mutations are rarely discovered clinically; several generations may pass before the
descendants of such a person mates with other heterozygotes.
Examples: Haemochromatosis, sickle cell anaemia, cystic fibrosis, Tay–Sachs disease,
phenylketonuria, 21-hydroxylase deficiency, albinism, mucopolysaccharidoses
(except Hunter syndrome), glycogenoses and galactosaemia.
Lysosomal storage diseases are a group of diseases in which the absence of degrad-
ing enzymes leads to accumulation of complex substrates (eg, sphingolipids and
mucopolysaccharides) in the lysosome.
Glycogenoses involve accumulation of glycogen in tissue due to increased synthesis or
decreased degradation of glycogen.
3. X-linked disorders
(a) All sex-linked disorders are X-linked; no Y-linked diseases are known.
(b) Most X-linked disorders are recessive.
(c) They are transmitted by heterozygous female carriers only to their sons.
(d) Heterozygous females rarely express the complete phenotype of the disease
as they have the paired normal allele. Due to inactivation of one of the
X chromosomes in females (Lyon’s hypothesis), it is possible for the normal
allele to be inactivated resulting in full expression of the disease in heterozy-
gote females.
(e) An affected male does not transmit the disease to his sons, but all his daughters are
carriers.
Examples: Lesch–Nyhan syndrome (hyperuricemia and self-mutilation due to defi-
ciency of HGPRT), fragile X syndrome (mental retardation), haemophilia, glucose-6
phosphate dehydrogenase deficiency, testicular feminization, chronic granulomatous
disease of childhood and Wiskott–Aldrich syndrome.
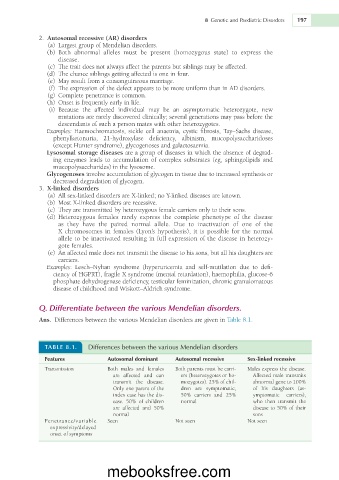
Q. Differentiate between the various Mendelian disorders.
Ans. Differences between the various Mendelian disorders are given in Table 8.1.
TABLE 8.1. Differences between the various Mendelian disorders
Features Autosomal dominant Autosomal recessive Sex-linked recessive
Transmission Both males and females Both parents must be carri- Males express the disease.
are affected and can ers (heterozygotes or ho- Affected male transmits
transmit the disease. mozygotes). 25% of chil- abnormal gene to 100%
Only one parent of the dren are symptomatic, of his daughters (as-
index case has the dis- 50% carriers and 25% ymptomatic carriers),
ease. 50% of children normal who then transmit the
are affected and 50% disease to 50% of their
normal sons
Penetrance/variable Seen Not seen Not seen
expressivity/delayed
onset of symptoms
mebooksfree.com