
Page 36 - 2021 Mid Year Open Enrollment Guide
P. 36
Dental Plans Vision Plans
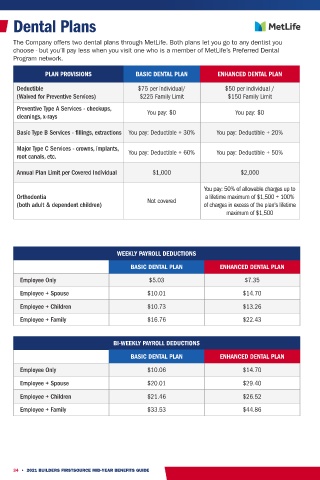
The Company offers two dental plans through MetLife. Both plans let you go to any dentist you We're committed to providing you with the best choices in eye doctors and corrective eyewear.
choose - but you’ll pay less when you visit one who is a member of MetLife’s Preferred Dental Frame and contact lens allowances can now be used in the same benefit year.
Program network.
PLAN PROVISIONS BASIC VISION PLAN ENHANCED VISION PLAN
PLAN PROVISIONS BASIC DENTAL PLAN ENHANCED DENTAL PLAN
In-Network
Deductible $75 per individual/ $50 per individual /
(Waived for Preventive Services) $225 Family Limit $150 Family Limit Exam (1x per calendar year) $10 copay $10 copay
Preventive Type A Services - checkups, $0 copay; 20% discount off
cleanings, x-rays You pay: $0 You pay: $0 35% discount off balance over $140 allowance
Frames (1x per calendar year)
Basic Type B Services - fillings, extractions You pay: Deductible + 30% You pay: Deductible + 20% retail price 40% discount off of additional
pairs of glasses
Major Type C Services - crowns, implants,
root canals, etc. You pay: Deductible + 60% You pay: Deductible + 50% Non-prescription sunglasses $50 discount off the purchase from Sunglass Hut
Standard Corrective Lenses (every 12 months)
Annual Plan Limit per Covered Individual $1,000 $2,000
Single Vision $50 copay $25 copay
Bifocal $70 copay $25 copay
You pay: 50% of allowable charges up to Trifocals $105 copay $25 copay
Orthodontia Not covered a lifetime maximum of $1,500 + 100% Lenticular N/A $25 copay
(both adult & dependent children) of charges in excess of the plan's lifetime
maximum of $1,500 Contact Lenses (Fit & Follow-up)
Standard (Disposable, Conventional, Daily) Plan pays up to $40 Plan pays up to $40
Premium (Toric, Multifocal, Cosmetic Color) 10% of retail price 10% of retail price
Contact Lenses (Materials Only)
WEEKLY PAYROLL DEDUCTIONS
Medically Necessary N/A $0 copay;
BASIC DENTAL PLAN ENHANCED DENTAL PLAN Cosmetic 15% discount off of retail 15% discount off of balance over
$140 allowance
Employee Only $5.03 $7.35
LASIK 15% discount off of retail or 5% off of promotional price
Employee + Spouse $10.01 $14.70
Discount for items not covered by the plan 20% discount
Employee + Children $10.73 $13.26
Employee + Family $16.76 $22.43 WEEKLY PAYROLL DEDUCTIONS
BASIC VISION PLAN ENHANCED VISION PLAN
BI-WEEKLY PAYROLL DEDUCTIONS
Employee Only $0.19 $1.09
BASIC DENTAL PLAN ENHANCED DENTAL PLAN Employee + Spouse $0.37 $2.08
Employee Only $10.06 $14.70 Employee + Children $0.43 $2.43
Employee + Family $0.63 $3.60
Employee + Spouse $20.01 $29.40
Employee + Children $21.46 $26.52 BI-WEEKLY PAYROLL DEDUCTIONS
Employee + Family $33.53 $44.86 BASIC VISION PLAN ENHANCED VISION PLAN
Employee Only $0.38 $2.19
Employee + Spouse $0.73 $4.16
Employee + Children $0.86 $4.86
Employee + Family $1.26 $7.19
34 • 2021 BUILDERS FIRSTSOURCE MID-YEAR BENEFITS GUIDE 2021 BUILDERS FIRSTSOURCE MID-YEAR BENEFITS GUIDE • 35