
Page 546 - fbkCardioDiabetes_2017
P. 546
522 Cardio Diabetes Medicine 2017
leviate symptoms and should be provided based on awaiting cardiac transplantation
the patient and family’s preferences.
As “palliative therapy” for symptom control in select
patients with stage D HF despite optimal GDMT and
WHEN TO USE? device therapy who are not eligible for either MCS or
cardiac transplantation.
TEMPORARY INTRAVENOUS INOTROPIC
SUPPORT WHEN NOT TO USE?
Patients with cardiogenic shock [6]should receive Use of parenteral inotropic agents in hospitalized pa-
temporary intravenous inotropic support to maintain tients is potentially harmful[6] if used
systemic perfusion and preserve end-organ perfor-
mance. • without documented severe systolic dysfunction,
Until definitive therapy (eg, coronary revasculariza- • without hypotension
tion, Mechanical Circulatory Support(MCS), heart • without impaired perfusion and
transplantation)
• without evidence of significantly depressed cardi-
Until resolution of the acute precipitating problem ac output, with or without congestion.
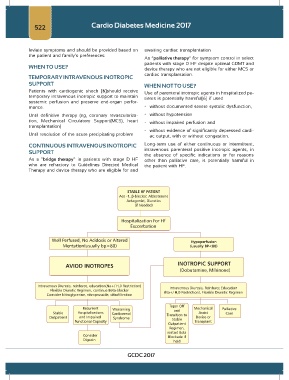
CONTINUOUS INTRAVENOUS INOTROPIC Long-term use of either continuous or intermittent,
SUPPORT intravenous parenteral positive inotropic agents, in
the absence of specific indications or for reasons
As a “bridge therapy” in patients with stage D HF other than palliative care, is potentially harmful in
who are refractory to Guidelines Directed Medical the patient with HF.
Therapy and device therapy who are eligible for and
GCDC 2017