
Page 1021 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1021
752 PART 5: Infectious Disorders
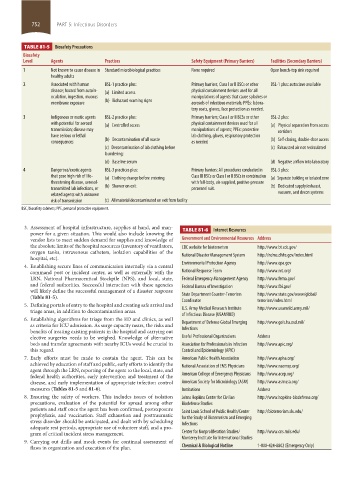
TABLE 81-5 Biosafety Precautions
Biosafety
Level Agents Practices Safety Equipment (Primary Barriers) Facilities (Secondary Barriers)
1 Not known to cause disease in Standard microbiological practices None required Open bench-top sink required
healthy adults
2 Associated with human BSL-1 practice plus: Primary barriers; Class I or II BSCs or other BSL-1 plus: autoclave available
disease; hazard from autoin- (a) Limited access physical containment devices used for all
oculation, ingestion, mucous manipulations of agents that cause splashes or
membrane exposure (b) Biohazard warning signs aerosols of infectious materials; PPEs: labora-
tory coats, gloves, face protection as needed.
3 Indigenous or exotic agents BSL-2 practice plus: Primary barriers; Class I or II BCSs or other BSL-2 plus:
with potential for aerosol (a) Controlled access physical containment devices used for all (a) Physical separation from access
transmission; disease may manipulations of agents; PPEs: protective corridors
have serious or lethal lab clothing, gloves, respiratory protection
consequences (b) Decontamination of all waste as needed (b) Self-closing, double-door access
(c) Decontamination of lab clothing before (c) Exhausted air not recirculated
laundering;
(d) Baseline serum (d) Negative airflow into laboratory
4 Dangerous/exotic agents BSL-3 practices plus: Primary barriers: All procedures conducted in BSL-3 plus:
that pose high risk of life- (a) Clothing change before entering Class III BSCs or Class I or II BSCs in combination (a) Separate building or isolated zone
threatening disease, aerosol- with full-body, air-supplied, positive-pressure
transmitted lab infections, or (b) Shower on exit personnel suit. (b) Dedicated supply/exhaust,
related agents with unknown vacuum, and decon systems
risk of transmission (c) All material decontaminated on exit from facility
BSC, biosafety cabinets; PPE, personal protective equipment.
3. Assessment of hospital infrastructure, supplies at hand, and man- TABLE 81-6 Internet Resources
power for a given situation. This would also include knowing the
vendor lists to meet sudden demand for supplies and knowledge of Government and Environmental Resources Address
the absolute limits of the hospital resources (inventory of ventilators, CDC website for bioterrorism http://www.bt.cdc.gov/
oxygen tanks, intravenous catheters, isolation capabilities of the National Disaster Management System http://ndms.dhhs.gov/index.html
hospital, etc).
4. Establishing secure lines of communication internally via a central Environmental Protection Agency http://www.epa.gov
command post or incident center, as well as externally with the National Response Team http://www.nrt.org/
LRN, National Pharmaceutical Stockpile (NPS), and local, state, Federal Emergency Management Agency http://www.fema.gov/
and federal authorities. Successful interaction with these agencies Federal Bureau of Investigation http://www.fbi.gov/
will likely define the successful management of a disaster response
(Table 81-5). State Department Counter-Terrorism http://www.state.gov/www/global/
Coordinator terrorism/index.html
5. Defining portals of entry to the hospital and creating safe arrival and
triage areas, in addition to decontamination areas. U.S. Army Medical Research Institute http://www.usamriid.army.mil/
of Infectious Disease (USAMRIID)
6. Establishing algorithms for triage from the ED and clinics, as well
as criteria for ICU admission. As surge capacity nears, the risks and Department of Defense Global Emerging http://www.geis.ha.osd.mil/
benefits of treating existing patients in the hospital and carrying out Infections
elective surgeries needs to be weighed. Knowledge of alternative Useful Professional Organizations Address
beds and transfer agreements with nearby ICUs would be crucial in Association for Professionals in Infection http://www.apic.org/
this regard. Control and Epidemiology (APIC)
7. Early efforts must be made to contain the agent. This can be American Public Health Association http://www.apha.org/
achieved by education of staff and public, early efforts to identify the National Association of EMS Physicians http://www.naemsp.org/
agent through the LRN, reporting of the agent to the local, state, and
federal health authorities, early intervention and treatment of the American College of Emergency Physicians http://www.acep.org/
disease, and early implementation of appropriate infection control American Society for Microbiology (ASM) http://www.asmusa.org/
measures (Tables 81-5 and 81-6). Institutions Address
8. Ensuring the safety of workers. This includes issues of isolation Johns Hopkins Center for Civilian http://www.hopkins-biodefense.org/
precautions, evaluation of the potential for spread among other Biodefense Studies
patients and staff once the agent has been confirmed, postexposure Saint Louis School of Public Health/Center http://bioterrorism.slu.edu/
prophylaxis, and vaccination. Staff exhaustion and posttraumatic for the Study of Bioterrorism and Emerging
stress disorder should be anticipated, and dealt with by scheduling Infections
adequate rest periods, appropriate use of volunteer staff, and a pro-
gram of critical incident stress management. Center for Nonproliferation Studies/ http://www.cns.miis.edu/
9. Carrying out drills and mock events for continual assessment of Monterey Institute for International Studies
flaws in organization and execution of the plan. Chemical & Biological Hotline 1-800-424-8802 (Emergency Only)
section05_c74-81.indd 752 1/23/2015 12:37:46 PM