
Page 2484 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 2484
2216 Part XIII Consultative Hematology
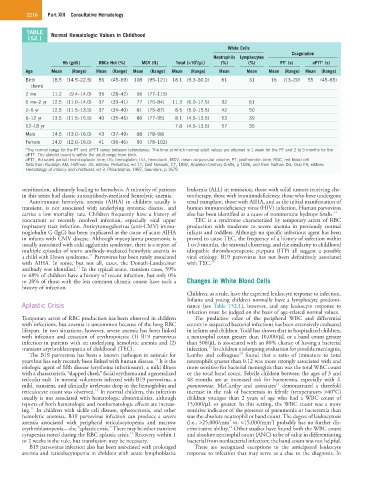
TABLE Normal Hematologic Values in Childhood
152.1
White Cells
Coagulation
Neutrophils Lymphocytes
Hb (g/dL) RBCs Hct (%) MCV (fL) Total (×10 /µL) (%) (%) PT (s) aPTT (s)
a
a
3
Age Mean (Range) Mean (Range) Mean (Range) Mean (Range) Mean Mean Mean (Range) Mean (Range)
Birth 18.5 (14.5–22.5) 56 (45–69) 108 (95–121) 18.1 (9.3–30.0) 61 31 16 (13–20) 55 (45–65)
(term)
2 mo 11.2 (9.4–14.0) 35 (28–42) 96 (77–115)
6 mo–2 yr 12.5 (11.0–14.0) 37 (33–41) 77 (70–84) 11.3 (6.0–17.5) 32 61
2–6 yr 12.5 (11.5–13.5) 37 (34–40) 81 (75–87) 8.5 (5.0–15.5) 42 50
6–12 yr 13.5 (11.5–15.5) 40 (35–45) 86 (77–95) 8.1 (4.5–13.5) 53 39
12–18 yr 7.8 (4.5–13.5) 57 35
Male 14.5 (13.0–16.0) 43 (37–49) 88 (78–98)
Female 14.0 (12.0–16.0) 41 (36–46) 90 (78–102)
a The normal range for the PT and aPTT varies between laboratories. The time at which normal adult values are attained is 1 week for the PT and 2 to 9 months for the
aPTT. The platelet count is within the adult range from birth.
aPTT, Activated partial thromboplastin time; Hb, hemoglobin; Hct, hematocrit; MCV, mean corpuscular volume; PT, prothrombin time; RBC, red blood cell.
Data from Rudolph AM, Hoffman JIE, editors: Pediatrics, ed 17, East Norwalk, CT, 1982, Appleton-Century-Crofts, p 1036, and from Nathan DG, Oski FA, editors:
Hematology of infancy and childhood, ed 3, Philadelphia, 1987, Saunders, p 1679.
sensitization, ultimately leading to hemolysis. A minority of patients leukemia (ALL) in remission, those with solid tumors receiving che-
in this series had classic autoantibody-mediated hemolytic anemia. motherapy, those with immunodeficiency, those who have undergone
Autoimmune hemolytic anemia (AIHA) in children usually is renal transplant, those with AIHA, and as the initial manifestation of
transient, is not associated with underlying systemic disease, and human immunodeficiency virus (HIV) infection. Human parvovirus
carries a low mortality rate. Children frequently have a history of also has been identified as a cause of nonimmune hydrops fetalis. 17
concurrent or recently resolved infection, especially viral upper TEC is a syndrome characterized by temporary arrest of RBC
respiratory tract infection. Anticytomegalovirus (anti-CMV) immu- production with moderate to severe anemia in previously normal
noglobulin G (IgG) has been implicated as the cause of acute AIHA infants and toddlers. Although no specific infectious agent has been
in infants with CMV disease. Although mycoplasma pneumonia is proved to cause TEC, the frequency of a history of infection within
usually associated with cold agglutinin syndrome, there is a report of 1 to 3 months, the seasonal clustering, and the similarity to childhood
multiple episodes of warm antibody-mediated hemolytic anemia in idiopathic thrombocytopenic purpura (ITP) all suggest a possible
11
a child with Down syndrome. Parvovirus has been rarely associated viral etiology. B19 parvovirus has not been definitively associated
with AIHA. In some, but not all, cases, the Donath-Landsteiner with TEC. 18
12
antibody was identified. In the typical acute, transient cases, 59%
to 68% of children have a history of recent infection, but only 0%
to 20% of those with the less common chronic course have such a Changes in White Blood Cells
history of infection.
Children, as a rule, have the expected leukocyte response to infection.
Infants and young children normally have a lymphocyte predomi-
Aplastic Crisis nance (see Table 152.1), however, and any leukocyte response to
infection must be judged on the basis of age-related normal values.
Temporary arrest of RBC production has been observed in children The predictive value of the peripheral WBC and differential
with infections, but anemia is uncommon because of the long RBC counts in suspected bacterial infections has been extensively evaluated
lifespan. In two situations, however, severe anemia has been linked in infants and children. Todd has shown that in hospitalized children,
with infection and cessation of erythropoiesis: (1) B19 parvovirus a neutrophil count greater than 10,000/µL or a band count greater
infection in patients with an underlying hemolytic anemia and (2) than 500/µL is associated with an 80% chance of having a bacterial
19
transient erythroblastopenia of childhood (TEC). infection. In children undergoing evaluation for possible meningitis,
20
The B19 parvovirus has been a known pathogen in animals for Lembo and colleagues found that a ratio of immature to total
13
years but has only recently been linked with human disease. It is the neutrophils greater than 0.12 was more strongly associated with and
etiologic agent of fifth disease (erythema infectiosum), a mild illness more sensitive for bacterial meningitis than was the total WBC count
with a characteristic “slapped cheek” facial erythema and a generalized or the total band count. Febrile children between the ages of 3 and
reticular rash. In normal volunteers infected with B19 parvovirus, a 48 months are at increased risk for bacteremia, especially with S.
21
mild, transient, and clinically irrelevant drop in the hemoglobin and pneumoniae. McCarthy and associates demonstrated a threefold
14
reticulocyte count was observed. In normal children, this infection increase in the risk of bacteremia in febrile (temperatures >40°C)
usually is not associated with hematologic abnormalities, although children younger than 2 years of age who had a WBC count of
reports of both hematologic and nonhematologic effects are increas- 15,000/µL or greater. In this setting, the WBC count was a more
15
ing. In children with sickle cell disease, spherocytosis, and other sensitive indicator of the presence of pneumonia or bacteremia than
hemolytic anemias, B19 parvovirus infection can produce a severe was the absolute neutrophil or band count. The degree of leukocytosis
2
2
anemia associated with peripheral reticulocytopenia and marrow (i.e., >25,000/mm vs. <15,000/mm ) probably has no further dis-
22
erythroblastopenia—the “aplastic crisis.” There may be other transient criminative ability. Other studies have found both the WBC count
16
cytopenias noted during the RBC aplastic crisis. Recovery within 1 and absolute neutrophil count (ANC) to be of value in differentiating
to 2 weeks is the rule, but transfusion may be necessary. bacterial from nonbacterial infection; the band count was not helpful.
B19 parvovirus infection also has been associated with prolonged There are recognized exceptions to the anticipated leukocyte
anemia and reticulocytopenia in children with acute lymphoblastic response to infection that may serve as a clue to the diagnosis. In