
Page 1664 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1664
CHAPTER 123: Critical Care of the Burn Patient 1183
Adult burn patients (>30 kg)
Protocol for fluid resuscitation Bar code label
Vitals unstable:
If burn >25%: Step one:
Add hetastarch Infuse LR at calculated rate HR >140, <60
at 20 mL/kg/24 h per Parkland protocol (below) BP <90/60
<90;
Start time:________ Measure urine output after 1 hour Sa O 2
Call physician
Vital signs stable: HR <140, BP >90/60, SaO >90
2
Urine Urine Urine Urine Urine
output output output output output
<15 mL 16-30 mL 31-50 mL 51-200 mL >201 mL
Increase IV Increase IV No change- Decrease IV Decrease IV
rate by 20% rate by 10% leave IV rate rate by 10% rate by 20%
initial rate initial rate as is initial rate initial rate
If urine output Urine output
<15 mL/h for >200 mL/h for
2 consecutive hours: 2 consecutive hours:
Call physician Call physician
Start hetastarch at
20 mL/kg/24 h
(if not started
previously)
Repeat Step one every hour until:
Calculated maintenance rate is reached
40 mL + dry weight (kg) =_________ total mL/hour
Admit weight:______.___kg
Burn size:_________.___%
Once at maintenance for 2 hours,
decrease hourly by 10% of initial rate until off Starting fluid rate:_____mL
Titrate by: __________mL
(10% of starting IVF rate)
Continue hourly UOP for 8 hours on burns >20% or
if otherwise indicated (difficult resuscitation, inhalation injury) Maintenance IVF Rate:
Wt (kg) + 40 = ___ mL/h
Parkland formula for
If urine output falls below 30 mL/h fluid resuscitation
return to Step one & call physician _____ kg × _____ × 4 =
(weight) (BSAB)
_______ mLs/1st24 hours
/2 = _______ mLs/1st8 hours
Obtain ABG, lactate, bladder pressure
/8 = _______ mLs/h IV rate
Do not include hetastarch, tube feedings, or medication fluids as part of the resuscitation fluids—
you should only titrate the LR during the resuscitation phase
Place this sheet in nurse manager’s mailbox when resuscitation is complete
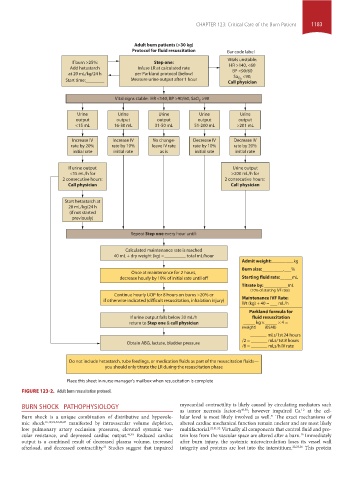
FIGURE 123-2. Adult burn resuscitation protocol.
BURN SHOCK PATHOPHYSIOLOGY myocardial contractility is likely caused by circulating mediators such
+2
as tumor necrosis factor-α 49,50 ; however impaired Ca at the cel-
Burn shock is a unique combination of distributive and hypovole- lular level is most likely involved as well. The exact mechanisms of
51
mic shock 16,19,22,32,46,47 manifested by intravascular volume depletion, altered cardiac mechanical function remain unclear and are most likely
low pulmonary artery occlusion pressures, elevated systemic vas- multifactorial. 22,51,52 Virtually all components that control fluid and pro-
cular resistance, and depressed cardiac output. 46,48 Reduced cardiac tein loss from the vascular space are altered after a burn. Immediately
16
output is a combined result of decreased plasma volume, increased after burn injury, the systemic microcirculation loses its vessel wall
afterload, and decreased contractility. Studies suggest that impaired integrity and proteins are lost into the interstitium. 22,25,26 This protein
21
section10.indd 1183 1/20/2015 9:21:33 AM