
Page 1666 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1666
CHAPTER 123: Critical Care of the Burn Patient 1185
B-1c Estimation of Burn & Diagram Date
Hosp No.
Name
Birthdate
Address
If not imprinted. Please print date, Hosp no., Name, Unit
Birth 1-4 5-9 10-14 15 Adult Burn
1 y Y Y Y Y size estimate
Head 19 17 13 11 9 7
Neck 2 2 2 2 2 2
Anterior trunk 13 13 13 13 13 13
R L L R
Posterior trunk 13 13 13 13 13 13
Right buttock 2.5 2.5 2.5 2.5 2.5 2.5
Left buttock 2.5 2.5 2.5 2.5 2.5 2.5
Genitalia 1 1 1 1 1 1
Right upper arm 4 4 4 4 4 4
Left upper arm 4 4 4 4 4 4
Right lower arm 3 3 3 3 3 3
Left lower arm 3 3 3 3 3 3
Right hand 2.5 2.5 2.5 2.5 2.5 2.5
Left hand 2.5 2.5 2.5 2.5 2.5 2.5
Patient’s
Right thigh 5.5 6.5 8 8.5 9 9.5
Left thigh 5.5 6.5 8 8.5 9 9.5
Wt.= _________ Ht.= ________ TBSA = _____.____ M 2
Right leg 5 5 5.5 6 6.5 7
Left leg 5 5 5.5 6 6.5 7
Adult fluid calculation Right foot 3.5 3.5 3.5 3.5 3.5 3.5
Wt. _________ Kg.
Left foot 3.5 3.5 3.5 3.5 3.5 3.5
× _____________ % BSAB
Total BSAB
× 4 = mL = _____________ mL/1st 24 hours
Patient arrival time (official) ____________________
/2 = _____________ mL/1st 8 hours
/8 = _____________ mL/hour IV rate Burn activation only Page sent at: _________
Signature of staff responding:
Additional notes:
Burn/Trauma faculty on call: _______________________________
Burn residents/LIP: ______________________________________
______________________________________________________
Trauma/Night float: _____________________________________
Anesthesia: ____________________________________________
RT: ___________________________________________________
Burn charge RN: ________________________________________
Signed and dated: _______________________/____/_____ Nursing: ______________________________________________
Signed and dated: _______________________/____/_____ ISS nursing supervisor: __________________________________
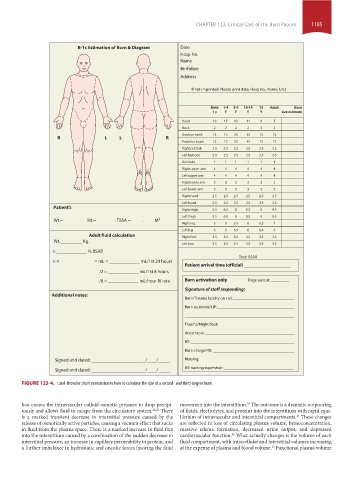
FIGURE 123-4. Lund-Browder chart demonstrates how to calculate the size of a second- and third-degree burn.
loss causes the intravascular colloid osmotic pressure to drop precipi- movement into the interstitium. The outcome is a dramatic outpouring
16
tously and allows fluid to escape from the circulatory system. 22,26 There of fluids, electrolytes, and proteins into the interstitium with rapid equi-
is a marked transient decrease in interstitial pressure caused by the librium of intravascular and interstitial compartments. These changes
25
release of osmotically active particles, causing a vacuum effect that sucks are reflected in loss of circulating plasma volume, hemoconcentration,
in fluid from the plasma space. There is a marked increase in fluid flux massive edema formation, decreased urine output, and depressed
into the interstitium caused by a combination of the sudden decrease in cardiovascular function. What actually changes is the volume of each
46
interstitial pressure, an increase in capillary permeability to protein, and fluid compartment, with intracellular and interstitial volumes increasing
25
a further imbalance in hydrostatic and oncotic forces favoring the fluid at the expense of plasma and blood volume. Functional plasma volume
section10.indd 1185 1/20/2015 9:21:35 AM