
Page 130 - fbkCardioDiabetes_2017
P. 130
106 Diabetic Cardiovascular Autonomic Neuropathy
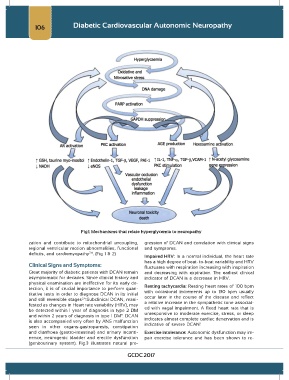
Fig1: Mechanisms that relate hyperglycemia to neuropathy
zation and contribute to mitochondrial uncoupling, gression of DCAN and correlation with clinical signs
regional ventricular motion abnormalities, functional and symptoms.
deficits, and cardiomyopathy . (Fig 1 & 2)
7,8
Impaired HRV: In a normal individual, the heart rate
has a high degree of beat- to-beat variability and HRV
Clinical Signs and Symptoms: fluctuates with respiration increasing with inspiration
Great majority of diabetic patients with DCAN remain and decreasing with expiration. The earliest clinical
asymptomatic for decades. Since clinical history and indicator of DCAN is a decrease in HRV.
physical examination are ineffective for its early de- Resting tachycardia: Resting heart rates of 100 bpm
tection, it is of crucial importance to perform quan- with occasional increments up to 130 bpm usually
titative tests in order to diagnose DCAN in its initial occur later in the course of the disease and reflect
2,4
and still reversible stages .Subclinical DCAN, mani- a relative increase in the sympathetic tone associat-
fested as changes in Heart rate variability (HRV), may ed with vagal impairment. A fixed heart rate that is
be detected within 1 year of diagnosis in type 2 DM unresponsive to moderate exercise, stress, or sleep
9
and within 2 years of diagnosis in type 1 DM . DCAN indicates almost complete cardiac denervation and is
is also accompanied very often by ANS malfunction indicative of severe DCAN .
1
seen in other organs-gastroparesis, constipation
and diarrhoea (gastro-intestinal) and urinary inconti- Exercise intolerance: Autonomic dysfunction may im-
nence, neurogenic bladder and erectile dysfunction pair exercise tolerance and has been shown to re-
(genitourinary system). Fig.3 illustrates natural pro-
GCDC 2017