
Page 131 - fbkCardioDiabetes_2017
P. 131
Cardio Diabetes Medicine 2017 107
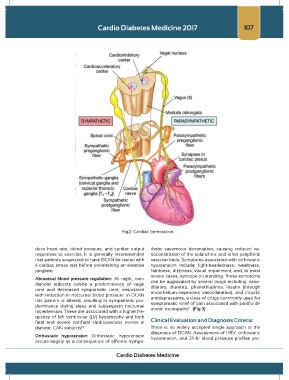
Fig2: Cardiac Innervation
duce heart rate, blood pressure, and cardiac output thetic vasomotor denervation, causing reduced va-
responses to exercise. It is generally recommended soconstriction of the splanchnic and other peripheral
that patients suspected to have DCAN be tested with vascular beds. Symptoms associated with orthostatic
a cardiac stress test before undertaking an exercise hypotension include: light-headedness, weakness,
program. faintness, dizziness, visual impairment, and, in most
severe cases, syncope on standing. These symptoms
Abnormal blood pressure regulation: At night, non- can be aggravated by several drugs including: vaso-
diabetic subjects exhibit a predominance of vagal dilators, diuretics, phenothiazines, insulin (through
tone and decreased sympathetic tone, associated endothelium-dependent vasodilatation), and tricyclic
with reduction in nocturnal blood pressure. In DCAN antidepressants, a class of drugs commonly used for
this pattern is altered, resulting in sympathetic pre- symptomatic relief of pain associated with painful di-
dominance during sleep and subsequent nocturnal abetic neuropathy . (Fig 3)
11
hypertension. These are associated with a higher fre-
quency of left ventricular (LV) hypertrophy and both
fatal and severe nonfatal cardiovascular events in Clinical Evaluation and Diagnosis Criteria:
diabetic CAN subjects . There is no widely accepted single approach to the
10
diagnosis of DCAN. Assessment of HRV, orthostatic
Orthostatic hypotension: Orthostatic hypotension hypotension, and 24-hr blood pressure profiles pro-
occurs largely as a consequence of efferent sympa-
Cardio Diabetes Medicine