
Page 178 - fbkCardioDiabetes_2017
P. 178
154 Stroke in Cardiodiabetic SyndromeHow different is it?
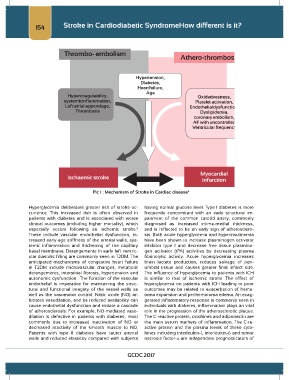
Pic 1 : Mechanism of Stroke in Cardiac disease 4
Hyperglycemia deliberates greater risk of stroke oc- having normal glucose level. Type I diabetes is more
currence. This increased risk is often observed in frequently concomitant with an early structural im-
patients with diabetes and is associated with worse pairment of the common carotid artery, commonly
clinical outcomes (including higher mortality), which diagnosed as increased intima-medial thickness,
especially occurs following an ischemic stroke. and is reflected to be an early sign of atherosclero-
5
These include vascular endothelial dysfunction, in- sis. Both acute hyperglycemia and hyperinsulinemia
creased early-age stiffness of the arterial walls, sys- have been shown to increase plasminogen activator
temic inflammation and thickening of the capillary inhibitor type 1 and decrease free tissue plasmino-
basal membrane. Derangements in early left ventric- gen activator (tPA) activities by decreasing plasma
ular diastolic filling are commonly seen in T2DM. The fibrinolytic activity. Acute hyperglycemia increases
anticipated mechanisms of congestive heart failure brain lactate production, reduces salvage of pen-
in T2DM include microvascular changes, metabolic umbral tissue and causes greater final infarct size.
derangements, interstitial fibrosis, hypertension and The influence of hyperglycemia to patients with ICH
autonomic dysfunction . The function of the vascular is similar to that of ischemic stroke. The effect of
endothelial is imperative for maintaining the struc- hyperglycemia on patients with ICH leading to poor
tural and functional integrity of the vessel walls as outcomes may be related to exacerbation of hema-
well as the vasomotor control. Nitric oxide (NO) ar- toma expansion and perihematoma edema. An exag-
bitrates vasodilation, and its reduced availability can gerated inflammatory response is commonly seen in
cause endothelial dysfunction and initiate a cascade individuals with diabetes, inflammation plays an vital
of atherosclerosis. For example, NO-mediated vaso- role in the progression of the atherosclerotic plaque.
dilation is defective in patients with diabetes, most The C-reactive protein, cytokines and adiponectin are
commonly due to increased inactivation of NO or the main serum markers of inflammation. The C-re-
decreased reactivity of the smooth muscle to NO. active protein and the plasma levels of these cyto-
Patients with type II diabetes have tauter arterial kines including interleukin-1, interleukin-6 and tumor
walls and reduced elasticity compared with subjects necrosis factor-α are independent prognosticators of
GCDC 2017