
Page 54 - fbkCardioDiabetes_2017
P. 54
30 Cardio Diabetes Medicine 2017
The New Brave World of Dyslipidemia :
Ready to Target ASCVD after Statins
Dr. P. C. Manoria,
MD., DM., FSACC., FESC.,
Director menoria Heart and critical care Hospital,
Former Prof and H.O.D Cardiology GMC,Bhopal.
Abstract is therefore poised to improve compliance greatly
With kicking off of second revolution of PCSK9 in- compared to PCSK9 MoAbs. It is obviously emerg-
hibition by fully humanized MoAbs after the statin ing as a very important competitor to PCSK9 MoAbs.
revolution, we are amidst a new brave world of dyslip- The future ongoing trials will tell us more about this
idemia which is ready to target atherosclerotic cardio- molecule.
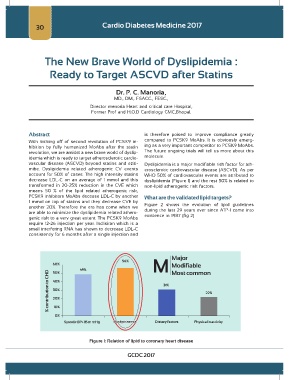
vascular disease (ASCVD) beyond statins and eziti- Dyslipidemia is a major modifiable risk factor for ath-
mibe. Dyslipidemia related atherogenic CV events erosclerotic cardiovascular disease (ASCVD). As per
account for 50% of cases. The high intensity statins WHO 50% of cardiovascular events are attributed to
decrease LDL-C on an average of 1 mmol and this dyslipidemia (Figure 1) and the rest 50% is related to
transformed in 20-25% reduction in the CVE which non-lipid atherogenic risk factors.
means 50 % of the lipid related atherogenic risk,
PCSK9 inhibitors MoAbs decease LDL-C by another What are the validated lipid targets?
1 mmol on top of statins and they decrease CVE by Figure 2 shows the evolution of lipid guidelines
another 20%. Therefore the era has come when we during the last 29 years ever since ATP-1 came into
are able to minimize the dyslipidemia related athero- existence in 1987 (fig 2)
genic risk to a very great extent. The PCSK9 MoAbs
require 12-26 injection per year. Inclisiran which is a
small interfering RNA has shown to decrease LDL-C
consistently for 6 months after a single injection and
Figure 1: Relation of lipid to coronary heart disease
GCDC 2017