
Page 314 - Critical Care Nursing Demystified
P. 314
Chapter 6 CARE OF THE TRAUMATIZED PATIENT 299
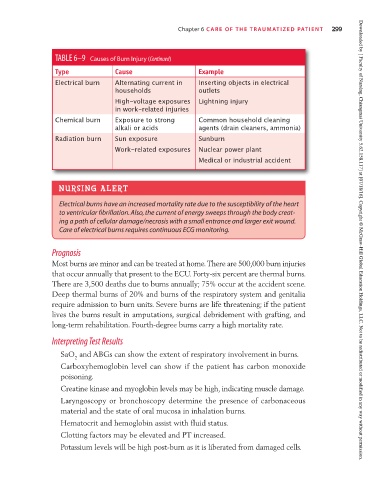
TABLE 6–9 Causes of Burn Injury (Continued)
Type Cause Example
Electrical burn Alternating current in Inserting objects in electrical
households outlets
High-voltage exposures Lightning injury
in work-related injuries
Chemical burn Exposure to strong Common household cleaning
alkali or acids agents (drain cleaners, ammonia)
Radiation burn Sun exposure Sunburn
Work-related exposures Nuclear power plant
Medical or industrial accident
NURSING ALERT
Electrical burns have an increased mortality rate due to the susceptibility of the heart
to ventricular fibrillation. Also, the current of energy sweeps through the body creat-
ing a path of cellular damage/necrosis with a small entrance and larger exit wound.
Care of electrical burns requires continuous ECG monitoring. Downloaded by [ Faculty of Nursing, Chiangmai University 5.62.158.117] at [07/18/16]. Copyright © McGraw-Hill Global Education Holdings, LLC. Not to be redistributed or modified in any way without permission.
Prognosis
Most burns are minor and can be treated at home. There are 500,000 burn injuries
that occur annually that present to the ECU. Forty-six percent are thermal burns.
There are 3,500 deaths due to burns annually; 75% occur at the accident scene.
Deep thermal burns of 20% and burns of the respiratory system and genitalia
require admission to burn units. Severe burns are life threatening; if the patient
lives the burns result in amputations, surgical debridement with grafting, and
long-term rehabilitation. Fourth-degree burns carry a high mortality rate.
Interpreting Test Results
SaO and ABGs can show the extent of respiratory involvement in burns.
2
Carboxyhemoglobin level can show if the patient has carbon monoxide
poisoning.
Creatine kinase and myoglobin levels may be high, indicating muscle damage.
Laryngoscopy or bronchoscopy determine the presence of carbonaceous
material and the state of oral mucosa in inhalation burns.
Hematocrit and hemoglobin assist with fluid status.
Clotting factors may be elevated and PT increased.
Potassium levels will be high post-burn as it is liberated from damaged cells.