
Page 372 - Critical Care Nursing Demystified
P. 372
Chapter 8 CARE OF THE PATIENT WITH CRITICAL RENAL NEEDS 357
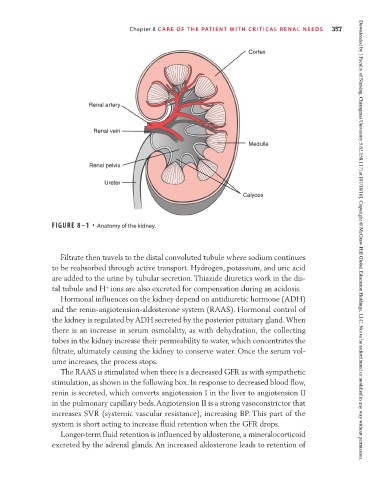
Cortex
Renal artery
Renal vein
Medulla
Renal pelvis
Ureter
Calyces
FIGURE 8–1 • Anatomy of the kidney. Downloaded by [ Faculty of Nursing, Chiangmai University 5.62.158.117] at [07/18/16]. Copyright © McGraw-Hill Global Education Holdings, LLC. Not to be redistributed or modified in any way without permission.
Filtrate then travels to the distal convoluted tubule where sodium continues
to be reabsorbed through active transport. Hydrogen, potassium, and uric acid
are added to the urine by tubular secretion. Thiazide diuretics work in the dis-
+
tal tubule and H ions are also excreted for compensation during an acidosis.
Hormonal influences on the kidney depend on antidiuretic hormone (ADH)
and the renin-angiotension-aldosterone system (RAAS). Hormonal control of
the kidney is regulated by ADH secreted by the posterior pituitary gland. When
there is an increase in serum osmolality, as with dehydration, the collecting
tubes in the kidney increase their permeability to water, which concentrates the
filtrate, ultimately causing the kidney to conserve water. Once the serum vol-
ume increases, the process stops.
The RAAS is stimulated when there is a decreased GFR as with sympathetic
stimulation, as shown in the following box. In response to decreased blood flow,
renin is secreted, which converts angiotension I in the liver to angiotension II
in the pulmonary capillary beds. Angiotension II is a strong vasoconstrictor that
increases SVR (systemic vascular resistance), increasing BP. This part of the
system is short acting to increase fluid retention when the GFR drops.
Longer-term fluid retention is influenced by aldosterone, a mineralocorticoid
excreted by the adrenal glands. An increased aldosterone leads to retention of