
Page 185 - Critical Care Notes
P. 185
4223_Tab06_175-198 29/08/14 8:27 AM Page 179
179
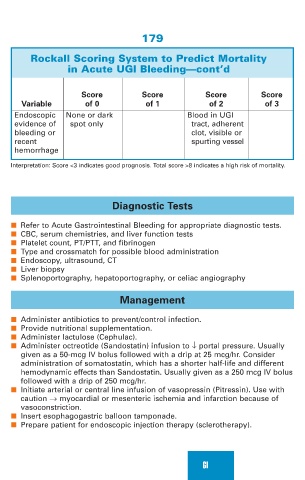
Rockall Scoring System to Predict Mortality
in Acute UGI Bleeding—cont’d
Score Score Score Score
Variable of 0 of 1 of 2 of 3
Endoscopic None or dark Blood in UGI
evidence of spot only tract, adherent
bleeding or clot, visible or
recent spurting vessel
hemorrhage
Interpretation: Score <3 indicates good prognosis. Total score >8 indicates a high risk of mortality.
Diagnostic Tests
■ Refer to Acute Gastrointestinal Bleeding for appropriate diagnostic tests.
■ CBC, serum chemistries, and liver function tests
■ Platelet count, PT/PTT, and fibrinogen
■ Type and crossmatch for possible blood administration
■ Endoscopy, ultrasound, CT
■ Liver biopsy
■ Splenoportography, hepatoportography, or celiac angiography
Management
■ Administer antibiotics to prevent/control infection.
■ Provide nutritional supplementation.
■ Administer lactulose (Cephulac).
■ Administer octreotide (Sandostatin) infusion to ↓ portal pressure. Usually
given as a 50-mcg IV bolus followed with a drip at 25 mcg/hr. Consider
administration of somatostatin, which has a shorter half-life and different
hemodynamic effects than Sandostatin. Usually given as a 250 mcg IV bolus
followed with a drip of 250 mcg/hr.
■ Initiate arterial or central line infusion of vasopressin (Pitressin). Use with
caution → myocardial or mesenteric ischemia and infarction because of
vasoconstriction.
■ Insert esophagogastric balloon tamponade.
■ Prepare patient for endoscopic injection therapy (sclerotherapy).
GI