
Page 1056 - Williams Hematology ( PDFDrive )
P. 1056
1030 Part VII: Neutrophils, Eosinophils, Basophils, and Mast Cells Chapter 66: Disorders of Neutrophil Function 1031
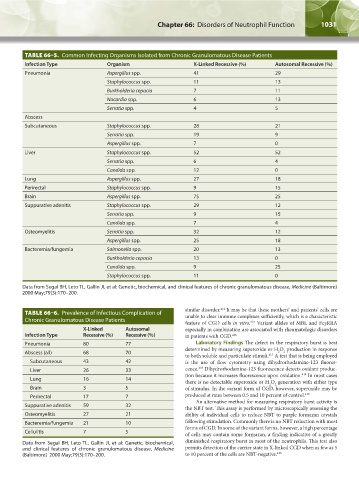
TABLE 66–5. Common Infecting Organisms Isolated from Chronic Granulomatous Disease Patients
Infection Type Organism X-Linked Recessive (%) Autosomal Recessive (%)
Pneumonia Aspergillus spp. 41 29
Staphylococcus spp. 11 13
Burkholderia cepacia 7 11
Nocardia spp. 6 13
Serratia spp. 4 5
Abscess
Subcutaneous Staphylococcus spp. 28 21
Serratia spp. 19 9
Aspergillus spp. 7 0
Liver Staphylococcus spp. 52 52
Serratia spp. 6 4
Candida spp. 12 0
Lung Aspergillus spp. 27 18
Perirectal Staphylococcus spp. 9 15
Brain Aspergillus spp. 75 25
Suppurative adenitis Staphylococcus spp. 29 12
Serratia spp. 9 15
Candida spp. 7 4
Osteomyelitis Serratia spp. 32 12
Aspergillus spp. 25 18
Bacteremia/fungemia Salmonella spp. 20 13
Burkholderia cepacia 13 0
Candida spp. 9 25
Staphylococcus spp. 11 0
Data from Segal BH, Leto TL, Gallin JI, et al: Genetic, biochemical, and clinical features of chronic granulomatous disease, Medicine (Baltimore)
2000 May;79(3):170–200.
similar disorder. It may be that these mothers’ and patients’ cells are
414
TABLE 66–6. Prevalence of Infectious Complication of unable to clear immune complexes sufficiently, which is a characteristic
Chronic Granulomatous Disease Patients feature of CGD cells in vitro. Variant alleles of MBL and FcγRIIA
415
X-Linked Autosomal especially in combination are associated with rheumatologic disorders
Infection Type Recessive (%) Recessive (%) in patients with CGD. 416
Pneumonia 80 77 Laboratory Findings The defect in the respiratory burst is best
determined by measuring superoxide or H O production in response
Abscess (all) 68 70 2 2
to both soluble and particulate stimuli. A test that is being employed
417
Subcutaneous 43 42 is the use of flow cytometry using dihydrorhodamine-123 fluores-
418
Liver 26 33 cence. Dihydrorhodamine-123 fluorescence detects oxidant produc-
tion because it increases fluorescence upon oxidation. In most cases
418
Lung 16 14
there is no detectable superoxide or H O generation with either type
2
2
Brain 3 5 of stimulus. In the variant form of CGD, however, superoxide may be
Perirectal 17 7 produced at rates between 0.5 and 10 percent of control. 419
An alternative method for measuring respiratory burst activity is
Suppurative adenitis 59 32
the NBT test. This assay is performed by microscopically assessing the
Osteomyelitis 27 21 ability of individual cells to reduce NBT to purple formazan crystals
Bacteremia/fungemia 21 10 following stimulation. Commonly there is no NBT reduction with most
forms of CGD. In some of the variant forms, however, a high percentage
Cellulitis 7 5 of cells may contain some formazan, a finding indicative of a greatly
Data from Segal BH, Leto TL, Gallin JI, et al: Genetic, biochemical, diminished respiratory burst in most of the neutrophils. This test also
and clinical features of chronic granulomatous disease, Medicine permits detection of the carrier state in X-linked CGD when as few as 5
(Baltimore) 2000 May;79(3):170–200. to 10 percent of the cells are NBT-negative. 420
Kaushansky_chapter 66_p1005-1042.indd 1031 9/21/15 10:48 AM