
Page 630 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 630
606 Part FIVE Allergic Diseases
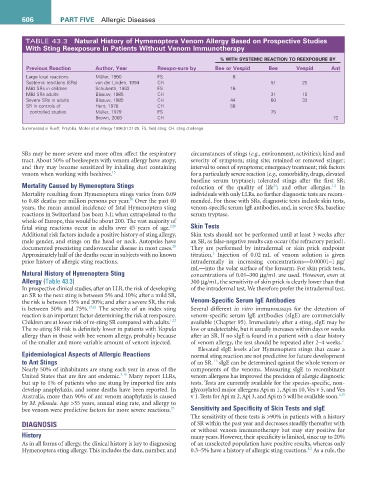
TABLE 43.3 Natural History of Hymenoptera Venom allergy Based on Prospective Studies
With Sting reexposure in Patients Without Venom Immunotherapy
% WItH SYStEMIC rEaCtION tO rEEXPOSUrE BY
Previous reaction author, Year reexpo-sure by Bee or Vespid Bee Vespid ant
Large local reactions Müller, 1990 FS 6
Systemic reactions (SRs) van der Linden, 1994 CH 51 25
Mild SRs in children Schuberth, 1983 FS 16
Mild SRs adults Blaauw, 1985 CH 31 10
Severe SRs in adults Blaauw, 1985 CH 44 60 33
SR in controls of Hunt, 1978 CH 58
controlled studies Müller, 1979 FS 75
Brown, 2003 CH 72
Summarized in Rueff, Przybilla, Müller et al Allergy 1996;51:21-25. FS, field sting; CH, sting challenge.
SRs may be more severe and more often affect the respiratory circumstances of stings (e.g., environment, activities); kind and
tract. About 50% of beekeepers with venom allergy have atopy, severity of symptom; sting site; retained or removed stinger;
and they may become sensitized by inhaling dust containing interval to onset of symptoms; emergency treatment; risk factors
venom when working with beehives. 15 for a particularly severe reaction (e.g., comorbidity, drugs, elevated
baseline serum tryptase); tolerated stings after the first SR;
Mortality Caused by Hymenoptera Stings reduction of the quality of life ; and other allergies. In
1,2
24
Mortality resulting from Hymenoptera stings varies from 0.09 individuals with only LLRs, no further diagnostic tests are recom-
20
to 0.48 deaths per million persons per year. Over the past 40 mended. For those with SRs, diagnostic tests include skin tests,
years, the mean annual incidence of fatal Hymenoptera sting venom-specific serum IgE antibodies, and, in severe SRs, baseline
reactions in Switzerland has been 3.1; when extrapolated to the serum tryptase.
whole of Europe, this would be about 200. The vast majority of
fatal sting reactions occur in adults over 45 years of age. 2,20 Skin Tests
Additional risk factors include a positive history of sting allergy, Skin tests should not be performed until at least 3 weeks after
male gender, and stings on the head or neck. Autopsies have an SR, as false-negative results can occur (the refractory period).
20
documented preexisting cardiovascular disease in most cases. They are performed by intradermal or skin prick endpoint
2
Approximately half of the deaths occur in subjects with no known titration. Injection of 0.02 mL of venom solution is given
prior history of allergic sting reactions. intradermally in increasing concentrations—0.00001–1 µg/
mL—into the volar surface of the forearm. For skin prick tests,
Natural History of Hymenoptera Sting concentrations of 0.01–300 µg/mL are used. However, even at
Allergy (Table 43.3) 300 µg/mL, the sensitivity of skin prick is clearly lower than that
In prospective clinical studies, after an LLR, the risk of developing of the intradermal test. We therefore prefer the intradermal test.
an SR to the next sting is between 5% and 10%; after a mild SR,
the risk is between 15% and 30%; and after a severe SR, the risk Venom-Specific Serum IgE Antibodies
is between 50% and 75%. 13,21 The severity of an index sting Several different in vitro immunoassays for the detection of
reaction is an important factor determining the risk at reexposure. venom-specific serum IgE antibodies (sIgE) are commercially
1,22
Children are at lower risk of re-sting SR compared with adults. available (Chapter 95). Immediately after a sting, sIgE may be
The re-sting SR risk is definitely lower in patients with Vespula low or undetectable, but it usually increases within days or weeks
allergy than in those with bee venom allergy, probably because after an SR. If no sIgE is found in a patient with a clear history
of the smaller and more variable amount of venom injected. of venom allergy, the test should be repeated after 2–4 weeks. 2
Elevated sIgE levels after Hymenoptera stings that cause a
Epidemiological Aspects of Allergic Reactions normal sting reaction are not predictive for future development
to Ant Stings of an SR. sIgE can be determined against the whole venom or
13
Nearly 50% of inhabitants are stung each year in areas of the components of the venoms. Measuring sIgE to recombinant
United States that are fire ant endemic. 3,10 Many report LLRs, venom allergens has improved the precision of allergic diagnostic
but up to 1% of patients who are stung by imported fire ants tests. Tests are currently available for the species-specific, non-
develop anaphylaxis, and some deaths have been reported. In glycosylated major allergens Api m 1, Api m 10, Ves v 5, and Ves
Australia, more than 90% of ant venom anaphylaxis is caused v 1. Tests for Api m 2, Api 3, and Api m 5 will be available soon. 6,25
by M. pilosula. Age >35 years, annual sting rate, and allergy to
bee venom were predictive factors for more severe reactions. 23 Sensitivity and Specificity of Skin Tests and sIgE
The sensitivity of these tests is >90% in patients with a history
DIAGNOSIS of SR within the past year and decreases steadily thereafter with
or without venom immunotherapy but may stay positive for
History many years. However, their specificity is limited, since up to 20%
As in all forms of allergy, the clinical history is key to diagnosing of an unselected population have positive results, whereas only
1,2
Hymenoptera sting allergy. This includes the date, number, and 0.3–5% have a history of allergic sting reactions. As a rule, the