
Page 646 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 646
CHaPter 44 Atopic and Contact Dermatitis 621
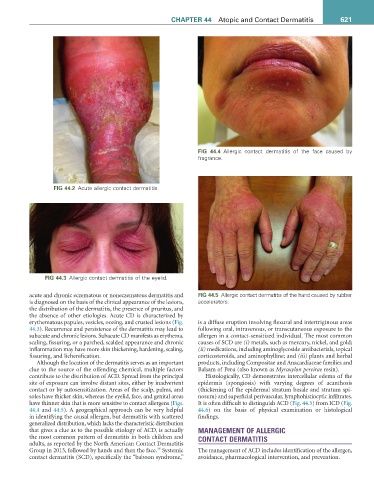
fiG 44.4 Allergic contact dermatitis of the face caused by
fragrance.
fiG 44.2 Acute allergic contact dermatitis.
fiG 44.3 Allergic contact dermatitis of the eyelid.
acute and chronic eczematous or noneczematous dermatitis and fiG 44.5 Allergic contact dermatitis of the hand caused by rubber
is diagnosed on the basis of the clinical appearance of the lesions, accelerators.
the distribution of the dermatitis, the presence of pruritus, and
the absence of other etiologies. Acute CD is characterized by
erythematous papules, vesicles, oozing, and crusted lesions (Fig. is a diffuse eruption involving flexural and intertriginous areas
44.3). Recurrence and persistence of the dermatitis may lead to following oral, intravenous, or transcutaneous exposure to the
subacute and chronic lesions. Subacute CD manifests as erythema, allergen in a contact-sensitized individual. The most common
scaling, fissuring, or a parched, scalded appearance and chronic causes of SCD are (i) metals, such as mercury, nickel, and gold;
inflammation may have more skin thickening, hardening, scaling, (ii) medications, including aminoglycoside antibacterials, topical
fissuring, and lichenification. corticosteroids, and aminophylline; and (iii) plants and herbal
Although the location of the dermatitis serves as an important products, including Compositae and Anacardiaceae families and
clue to the source of the offending chemical, multiple factors Balsam of Peru (also known as Myroxylon pereirae resin).
contribute to the distribution of ACD. Spread from the principal Histologically, CD demonstrates intercellular edema of the
site of exposure can involve distant sites, either by inadvertent epidermis (spongiosis) with varying degrees of acanthosis
contact or by autosensitization. Areas of the scalp, palms, and (thickening of the epidermal stratum basale and stratum spi-
soles have thicker skin, whereas the eyelid, face, and genital areas nosum) and superficial perivascular, lymphohistiocytic infiltrates.
have thinner skin that is more sensitive to contact allergens (Figs. It is often difficult to distinguish ACD (Fig. 44.5) from ICD (Fig.
44.4 and 44.5). A geographical approach can be very helpful 44.6) on the basis of physical examination or histological
in identifying the causal allergen, but dermatitis with scattered findings.
generalized distribution, which lacks the characteristic distribution
that gives a clue as to the possible etiology of ACD, is actually MANAGEMENT OF ALLERGIC
the most common pattern of dermatitis in both children and CONTACT DERMATITIS
adults, as reported by the North American Contact Dermatitis
48
Group in 2013, followed by hands and then the face. Systemic The management of ACD includes identification of the allergen,
contact dermatitis (SCD), specifically the “baboon syndrome,” avoidance, pharmacological intervention, and prevention.