
Page 838 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 838
810 Part SIX Systemic Immune Diseases
Vascular component Extravascular component
Granulomatous, transmural intense acute phase response
inflammation (IL-6, SAA, CRP, ESR, etc)
dendritic cells, CD4 T cells, myalgias
macrophages, giant cells, etc malaise, anorexia, fever
Giant cell
arteritis
Vessel wall remodeling
Aorta: dissection, wall damage,
aneurysm, rupture Age of the host
Branches: intimal hyperplasia,
luminal occlusion GCA/PMR: >50 yrs
TA: <40 yrs
Tissue tropism
th
GCA: Aorta + 3-5 branches
axillary, temporal, ophthalmic, etc
st
nd
TA: Aorta + 1 and 2 branches
subclavian, carotid, mesenteric, renal, etc
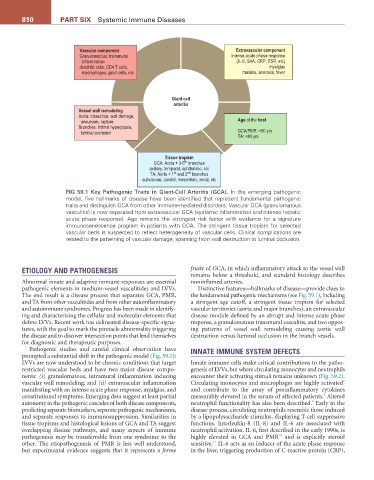
FIG 59.1 Key Pathogenic Traits in Giant-Cell Arteritis (GCA). In the emerging pathogenic
model, five hallmarks of disease have been identified that represent fundamental pathogenic
traits and distinguish GCA from other immune-mediated disorders. Vascular GCA (granulomatous
vasculitis) is now separated from extravascular GCA (systemic inflammation and intense hepatic
acute phase response). Age remains the strongest risk factor with evidence for a signature
immunosenescence program in patients with GCA. The stringent tissue tropism for selected
vascular beds is suspected to reflect heterogeneity of vascular cells. Clinical complications are
related to the patterning of vascular damage, spanning from wall destruction to luminal occlusion.
ETIOLOGY AND PATHOGENESIS fruste of GCA, in which inflammatory attack to the vessel wall
remains below a threshold, and standard histology describes
Abnormal innate and adaptive immune responses are essential noninflamed arteries.
pathogenic elements in medium-vessel vasculitides and LVVs. Distinctive features—hallmarks of disease—provide clues to
The end result is a disease process that separates GCA, PMR, the fundamental pathogenic mechanisms (see Fig. 59.1), including
and TA from other vasculitides and from other autoinflammatory a stringent age cutoff, a stringent tissue tropism for selected
and autoimmune syndromes. Progress has been made in identify- vascular territories (aorta and major branches), an extravascular
ing and characterizing the cellular and molecular elements that disease module defined by an abrupt and intense acute phase
define LVVs. Recent work has delineated disease-specific signa- response, a granulomatous transmural vasculitis, and two oppos-
tures, with the goal to mark the pinnacle abnormality triggering ing patterns of vessel wall remodeling causing aortic wall
the disease and to discover intersection points that lend themselves destruction versus luminal occlusion in the branch vessels.
for diagnostic and therapeutic purposes.
Pathogenic studies and careful clinical observation have INNATE IMMUNE SYSTEM DEFECTS
prompted a substantial shift in the pathogenic model (Fig. 59.1):
LVVs are now understood to be chronic conditions that target Innate immune cells make critical contributions to the patho-
restricted vascular beds and have two major disease compo- genesis of LVVs, but where circulating monocytes and neutrophils
nents: (i) granulomatous, intramural inflammation inducing encounter their activating stimuli remains unknown (Fig. 59.2).
7
vascular wall remodeling; and (ii) extravascular inflammation Circulating monocytes and macrophages are highly activated
manifesting with an intense acute phase response, myalgias, and and contribute to the array of proinflammatory cytokines
8
constitutional symptoms. Emerging data suggest at least partial measurably elevated in the serum of affected patients. Altered
9
autonomy in the pathogenic cascades of both disease components, neutrophil functionality has also been described. Early in the
predicting separate biomarkers, separate pathogenic mechanisms, disease process, circulating neutrophils resemble those induced
and separate responses to immunosuppression. Similarities in by a lipopolysaccharide stimulus, displaying T-cell suppressive
tissue tropisms and histological lesions of GCA and TA suggest functions. Interleukin-8 (IL-8) and IL-6 are associated with
overlapping disease pathways, and many aspects of immune neutrophil activation. IL-6, first described in the early 1990s, is
10
pathogenesis may be transferrable from one syndrome to the highly elevated in GCA and PMR and is explicitly steroid
11
other. The etiopathogenesis of PMR is less well understood, sensitive. IL-6 acts as an inducer of the acute phase response
but experimental evidence suggests that it represents a forme in the liver, triggering production of C-reactive protein (CRP),