
Page 472 - Clinical Hematology_ Theory _ Procedures ( PDFDrive )
P. 472
456 PART 6 ■ Neoplastic Disorders
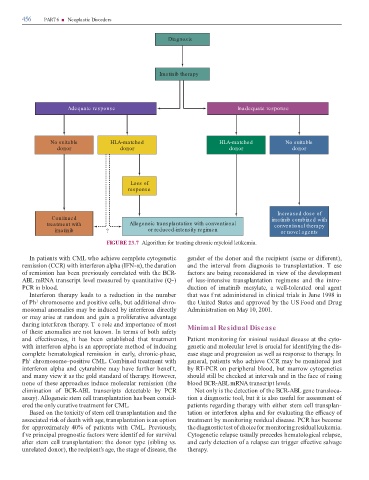
Diagnosis
Imatinib therapy
Adequate response Inadequate response
No suitable HLA-matched HLA-matched No suitable
donor donor donor donor
Loss of
response
Increased dose of
Continued imatinib combined with
treatment with Allogeneic transplantation with conventional conventional therapy
imatinib ? or reduced-intensity regimen or novel agents
FIGURE 23.7 Algorith or tre ting chronic yeloi leuke i .
In p tients with CML who chieve co plete cytogenetic gen er o the onor n the recipient (s e or i erent),
re ission (CCR) with inter eron lph (IFN-α), the ur tion n the interv l ro i gnosis to tr nspl nt tion. T ese
o re ission h s been previously correl te with the BCR- ctors re being reconsi ere in view o the evelop ent
ABL RNA tr nscript level e sure by qu ntit tive (Q-) o less-intensive tr nspl nt tion regi ens n the intro-
PCR in bloo . uction o i tinib esyl te, well-toler te or l gent
Inter eron ther py le s to re uction in the nu ber th t w s f rst inistere in clinic l tri ls in June 1998 in
o Ph chro oso e n positive cells, but ition l chro- the Unite St tes n pprove by the US Foo n Drug
1
oso l no lies y be in uce by inter eron irectly A inistr tion on M y 10, 2001.
or y rise t r n o n g in proli er tive v nt ge
uring inter eron ther py. T e role n i port nce o ost Minimal Residual Disease
o these no lies re not known. In ter s o both s ety
n e ectiveness, it h s been est blishe th t tre t ent P tient onitoring or minimal residual disease t the cyto-
with inter eron lph is n ppropri te etho o in ucing genetic n olecul r level is cruci l or i enti ying the is-
co plete he tologic l re ission in e rly, chronic-ph se, e se st ge n progression s well s response to ther py. In
Ph chro oso e–positive CML. Co bine tre t ent with gener l, p tients who chieve CCR y be onitore just
1
inter eron lph n cyt r bine y h ve urther benef t, by R -PCR on peripher l bloo , but rrow cytogenetics
n ny view it s the gol st n r o ther py. However, shoul still be checke t interv ls n in the ce o rising
none o these ppro ches in uce olecul r re ission (the bloo BCR-ABL mRNA tr nscript levels.
eli in tion o BCR-ABL tr nscripts etect ble by PCR Not only is the etection o the BCR-ABL gene tr nsloc -
ss y). Allogeneic ste cell tr nspl nt tion h s been consi - tion i gnostic tool, but it is lso use ul or ssess ent o
ere the only cur tive tre t ent or CML. p tients reg r ing ther py with either ste cell tr nspl n-
B se on the toxicity o ste cell tr nspl nt tion n the t tion or inter eron lph n or ev lu ting the e c cy o
ssoci te risk o e th with ge, tr nspl nt tion is n option tre t ent by onitoring resi u l ise se. PCR h s beco e
or pproxi tely 40% o p tients with CML. Previously, the i gnostic test o choice or onitoring resi u l leuke i .
f ve princip l prognostic ctors were i entif e or surviv l Cytogenetic rel pse usu lly prece es he tologic l rel pse,
er ste cell tr nspl nt tion: the onor type (sibling vs. n e rly etection o rel pse c n trigger e ective s lv ge
unrel te onor), the recipient’s ge, the st ge o ise se, the ther py.