
Page 27 - 2020 Benefits Guide
P. 27
To locate a provider near you, call
1-866-939-3633 or go to
www.enrollwitheyemed.com/access
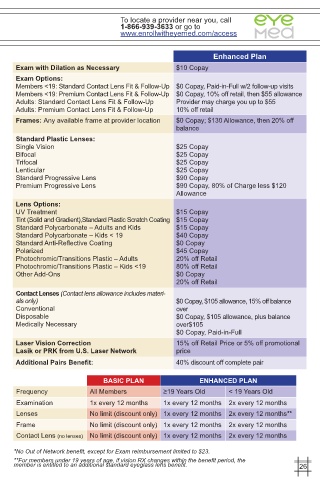
Enhanced Plan
Exam with Dilation as Necessary $10 Copay
Exam Options:
Members <19: Standard Contact Lens Fit & Follow-Up $0 Copay, Paid-in-Full w/2 follow-up visits
Members <19: Premium Contact Lens Fit & Follow-Up $0 Copay, 10% off retail, then $55 allowance
Adults: Standard Contact Lens Fit & Follow-Up Provider may charge you up to $55
Adults: Premium Contact Lens Fit & Follow-Up 10% off retail
Frames: Any available frame at provider location $0 Copay; $130 Allowance, then 20% off
balance
Standard Plastic Lenses:
Single Vision $25 Copay
Bifocal $25 Copay
Trifocal $25 Copay
Lenticular $25 Copay
Standard Progressive Lens $90 Copay
Premium Progressive Lens $90 Copay, 80% of Charge less $120
Allowance
Lens Options:
UV Treatment $15 Copay
Tint (Solid and Gradient),Standard Plastic Scratch Coating $15 Copay
Standard Polycarbonate – Adults and Kids $15 Copay
Standard Polycarbonate – Kids < 19 $40 Copay
Standard Anti-Reflective Coating $0 Copay
Polarized $45 Copay
Photochromic/Transitions Plastic – Adults 20% off Retail
Photochromic/Transitions Plastic – Kids <19 80% off Retail
Other Add-Ons $0 Copay
20% off Retail
Contact Lenses (Contact lens allowance includes materi-
als only) $0 Copay, $105 allowance, 15% off balance
Conventional over
Disposable $0 Copay, $105 allowance, plus balance
Medically Necessary over$105
$0 Copay, Paid-in-Full
Laser Vision Correction 15% off Retail Price or 5% off promotional
Lasik or PRK from U.S. Laser Network price
Additional Pairs Benefit: 40% discount off complete pair
BASIC PLAN ENHANCED PLAN
Frequency All Members ≥19 Years Old < 19 Years Old
Examination 1x every 12 months 1x every 12 months 2x every 12 months
Lenses No limit (discount only) 1x every 12 months 2x every 12 months**
Frame No limit (discount only) 1x every 12 months 2x every 12 months
Contact Lens (no lenses) No limit (discount only) 1x every 12 months 2x every 12 months
*No Out of Network benefit, except for Exam reimbursement limited to $23.
**For members under 19 years of age, if vision RX changes within the benefit period, the
member is entitled to an additional standard eyeglass lens benefit. 26