
Page 33 - 2021 Team Member Benefit Guide - English
P. 33
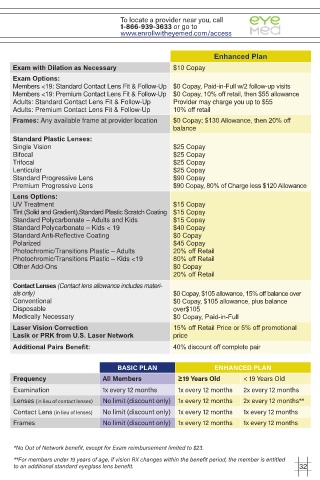
To locate a provider near you, call
1-866-939-3633 or go to
www.enrollwitheyemed.com/access
Enhanced Plan
Exam with Dilation as Necessary $10 Copay
Exam Options:
Members <19: Standard Contact Lens Fit & Follow-Up $0 Copay, Paid-in-Full w/2 follow-up visits
Members <19: Premium Contact Lens Fit & Follow-Up $0 Copay, 10% off retail, then $55 allowance
Adults: Standard Contact Lens Fit & Follow-Up Provider may charge you up to $55
Adults: Premium Contact Lens Fit & Follow-Up 10% off retail
Frames: Any available frame at provider location $0 Copay; $130 Allowance, then 20% off
balance
Standard Plastic Lenses:
Single Vision $25 Copay
Bifocal $25 Copay
Trifocal $25 Copay
Lenticular $25 Copay
Standard Progressive Lens $90 Copay
Premium Progressive Lens $90 Copay, 80% of Charge less $120 Allowance
Lens Options:
UV Treatment $15 Copay
Tint (Solid and Gradient),Standard Plastic Scratch Coating $15 Copay
Standard Polycarbonate – Adults and Kids $15 Copay
Standard Polycarbonate – Kids < 19 $40 Copay
Standard Anti-Reflective Coating $0 Copay
Polarized $45 Copay
Photochromic/Transitions Plastic – Adults 20% off Retail
Photochromic/Transitions Plastic – Kids <19 80% off Retail
Other Add-Ons $0 Copay
20% off Retail
Contact Lenses (Contact lens allowance includes materi-
als only) $0 Copay, $105 allowance, 15% off balance over
Conventional $0 Copay, $105 allowance, plus balance
Disposable over$105
Medically Necessary $0 Copay, Paid-in-Full
Laser Vision Correction 15% off Retail Price or 5% off promotional
Lasik or PRK from U.S. Laser Network price
Additional Pairs Benefit: 40% discount off complete pair
BASIC PLAN ENHANCED PLAN
Frequency All Members ≥19 Years Old < 19 Years Old
Examination 1x every 12 months 1x every 12 months 2x every 12 months
Lenses (in lieu of contact lenses) No limit (discount only) 1x every 12 months 2x every 12 months**
Contact Lens (in lieu of lenses) No limit (discount only) 1x every 12 months 1x every 12 months
Frames No limit (discount only) 1x every 12 months 1x every 12 months
*No Out of Network benefit, except for Exam reimbursement limited to $23.
**For members under 19 years of age, if vision RX changes within the benefit period, the member is entitled
to an additional standard eyeglass lens benefit. 32