
Page 695 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 695
514 PART 4: Pulmonary Disorders
ventricular heave, or jugular venous pressure elevation, indicating the
presence of pulmonary hypertension. 3
■ RESPIRATORY MECHANICS
Kyphoscoliosis reduces total lung capacity (TLC) and functional
residual capacity (FRC) (Fig. 58-2). Residual volume (RV) may be
normal or decreased to a lesser extent than FRC. Vital capacity (VC),
inspiratory capacity (IC = TLC − FRC), and expiratory reserve
volume (ERV = FRC − RV) are all decreased. Interestingly, pul-
13
monary function in adolescents is only weakly related to the angle
of scoliosis. In these patients, VC is also influenced by the degree
6
of thoracic kyphosis, location of the curve, and number of vertebral
bodies involved. Furthermore, spinal column rotation, respiratory
14
90° muscle strength, and duration of the curve are not clearly related to
pulmonary function in these patients. It does appear that age-related
decreases in chest wall compliance increase the risk of developing
ventilatory failure. 12,15
Patients with fibrothorax or thoracoplasty have similar abnormalities. 1,16-18
By contrast, obesity mainly reduces FRC and ERV and lesser changes in
RV, VC, or TLC. 19-21 In patients with ankylosing spondylitis, ERV and IC
excursions are restricted around a normal FRC, such that RV increases
and TLC decreases to reduce VC, a pattern similar to that seen in neu-
romuscular diseases of the chest wall. 22-27
In each of these disorders, it is the chest wall that limits the excur-
sion of the respiratory system; the lungs and respiratory muscles are
affected secondarily and to a lesser degree. In health, TLC is largely
determined by the pressure-volume (P-V) curve of the lung, but in KS
the P-V curve of the noncompliant chest wall dominates, lowering TLC
and FRC while RV is relatively spared (Fig. 58-3). Note that the P-V
curve of the respiratory system is shifted downward and to the right,
requiring patients to work harder for each tidal breath. Normal lung
compliance and respiratory muscle strength are assumed in Figure 58-3,
although reductions in both contribute to low lung volumes in selected
patients with either parenchymal lung disease or neuromuscular
FIGURE 58-1. Determination of the scoliotic angle by the Cobb method. The scoliotic defor- dysfunction. Indeed, in four patients with severe KS requiring mechan-
mity consists of a primary initiating curve and a secondary compensatory curve. The scoliotic angle ical ventilation for acute respiratory failure, both lung and chest wall
is commonly determined by the intersection of lines estimating the position of the upper and compliance were decreased. Decreased lung compliance may occur
28
lower components of the primary curve. (Reproduced with permission from Grippi MA, Fishman as a result of infection, edema, atelectasis, or abnormalities in alveo-
AP. Respiratory failure in structural and neuromuscular disorders involving the chest bellows. In: lar surface tension and may respond to positive-pressure ventilation
Fishman AP, ed. Pulmonary Diseases and Disorders. 2nd ed. New York, NY: McGraw-Hill; 1988.) (see below). 29
Inspiratory muscle dysfunction occurs when the deformed thorax
Thoracic deformity with loss of height and asymmetric chest wall excur- places inspiratory muscles at a mechanical disadvantage or there is respi-
sions often dominates the physical exam findings. Chest auscultation ratory muscle fatigue. 30,31 When KS is a manifestation of neuromuscular
may reveal crackles or coarse wheezes from atelectasis and failure to disease (eg, postpolio syndrome), inspiratory muscles may be affected
clear secretions. Cardiac examination may demonstrate a loud P , right directly by the neuromuscular disease.
2
8
Normal
TLC Obesity
6 IC VC Ankylosing
Lung volume (liters) 4 scoliosis Pulmonary
spondylitis
Kypho-
fibrosis
2
FRC ERV
RV
0
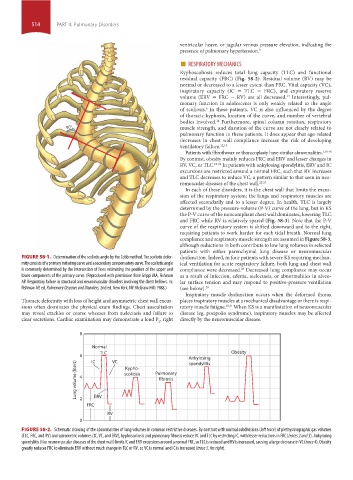
FIGURE 58-2. Schematic drawing of the abnormalities of lung volumes in common restrictive diseases. By contrast with normal subdivisions (left trace) of plethysmographic gas volumes
(TLC, FRC, and RV) and spirometric volumes (IC, VC, and ERV), kyphoscoliosis and pulmonary fibrosis reduce VC and TLC by restricting IC, with lesser reductions in FRC (traces 2 and 3). Ankylosing
spondylitis (like neuromuscular diseases of the chest wall) limits IC and ERV excursions around a normal FRC, so TLC is reduced and RV is increased, causing a large decrease in VC (trace 4). Obesity
greatly reduces FRC to eliminate ERV without much change in TLC or RV, so VC is normal and IC is increased (trace 5, far right).
section04.indd 514 1/23/2015 2:20:27 PM