
Page 152 - Psychology of Wounds and Wound Care in Clinical Practice ( PDFDrive )
P. 152
Diabetic Foot Ulcer (DFU) 127
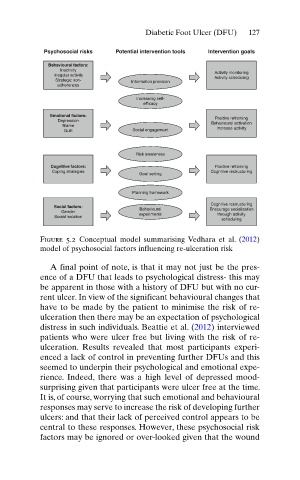
Psychosocial risks Potential intervention tools Intervention goals
Behavioural factors:
Inactivity
Activity monitoring
Irregular activity Activity scheduling
Strategic non- Information provision
adherences
Increasing self-
efficacy
Emotional factors:
Positive reframing
Depression
Behavioural activation
Blame Increase activity
Guilt Social engagement
Risk awareness
Cognitive factors: Positive reframing
Coping strategies Cognitive restructuring
Goal setting
Planning homework
Cognitive restructuring
Social factors: Behavioural Encourage socialisation
Gender
Social isolation experiments through activity
scheduling
Figure 5.2 Conceptual model summarising Vedhara et al. ( 2012 )
model of psychosocial factors influencing re-ulceration risk
A final point of note, is that it may not just be the pres-
ence of a DFU that leads to psychological distress- this may
be apparent in those with a history of DFU but with no cur-
rent ulcer. In view of the significant behavioural changes that
have to be made by the patient to minimise the risk of re-
ulceration then there may be an expectation of psychological
distress in such individuals. Beattie et al. ( 2012 ) interviewed
patients who were ulcer free but living with the risk of re-
ulceration. Results revealed that most participants experi-
enced a lack of control in preventing further DFUs and this
seemed to underpin their psychological and emotional expe-
rience. Indeed, there was a high level of depressed mood-
surprising given that participants were ulcer free at the time.
It is, of course, worrying that such emotional and behavioural
responses may serve to increase the risk of developing further
ulcers: and that their lack of perceived control appears to be
central to these responses. However, these psychosocial risk
factors may be ignored or over-looked given that the wound