
Page 120 - Critical Care Notes
P. 120
4223_Tab03_107-130 29/08/14 8:28 AM Page 114
RESP
■ Use silver- or antimicrobial-coated ETTs if patient is mechanically ventilated
>48 hr.
■ Use a subglottic secretion drainage system (CASS). Intermittent aspiration
preferred over continuous aspiration of subglottic secretions.
■ Consider Mucus Shaver or Mucus Slurper to clean inner lumen of ETT of
secretions and biofilm.
■ Maintain ETT cuff pressures at ≥20 mm Hg. Check cuff pressures every
8 hr. Consider a pneumatic device that will maintain ETT cuff inflating
pressure.
■ Eliminate routine saline bronchial lavage during ETT suctioning.
■ Drain condensation in ventilator tubing down and away from patient.
■ The practice of routine suctioning every 4 hr is being questioned. Do suction
as needed. Replace all suction equipment every 24 hr.
■ Provide “sedation vacations” at least once every 24 hr. Slowly decrease
amount and frequency of sedation.
■ Assess readiness to extubate, and extubate as soon as possible.
■ Establish spontaneous breathing trials and protocols.
■ Discontinue mechanical ventilation as soon as possible. Consider
noninvasive ventilation (NIV) such as BiPAP and CPAP.
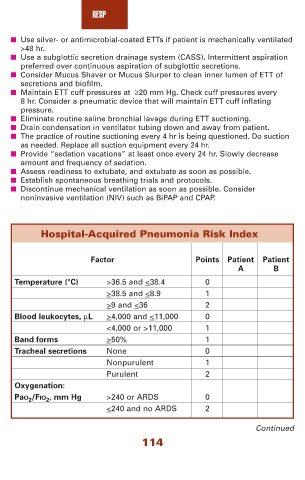
Hospital-Acquired Pneumonia Risk Index
Factor Points Patient Patient
A B
Temperature (°C) >36.5 and <38.4 0
>38.5 and <8.9 1
>9 and <36 2
Blood leukocytes, μL >4,000 and <11,000 0
<4,000 or >11,000 1
Band forms >50% 1
Tracheal secretions None 0
Nonpurulent 1
Purulent 2
Oxygenation:
PaO 2 /FIO 2 , mm Hg >240 or ARDS 0
<240 and no ARDS 2
Continued
114