
Page 172 - Cardiac Nursing
P. 172
8:2
009
9/2
5 A
P
P
M
52.
p13
2-1
52.
9/0
0
qxd
0-c
K34
ara
06_
LWBK340-c06_06_p132-152.qxd 09/09/2009 08:25 AM Page 148 Aptara
L L LWB K34 0-c 06_ p13 2-1 52. qxd 0 9/0 9/2 009 0 0 8:2 5 A M P a a g e 1 48 Apt ara
K34
LWB
48
Apt
48
g
e 1
148 PA R T I I / Physiologic and Pathologic Responses
Obstruction Neurohumoral
Decreased Pressure load
RV CCP
Wall tension Decreased
O demand RV output
2
Ischemia RV Decompensation
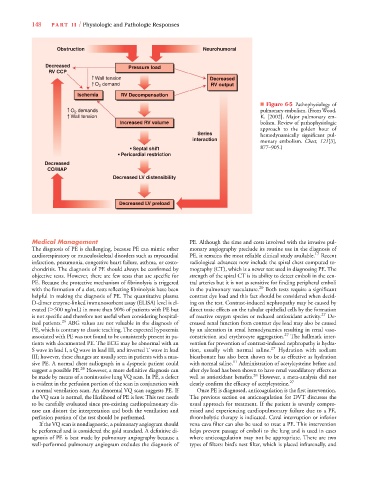
■ Figure 6-5 Pathophysiology of
O demands pulmonary embolism. (From Wood,
2
Wall tension K. [2002]. Major pulmonary em-
Increased RV volume bolism. Review of pathophysiologic
approach to the golden hour of
Series hemodynamically significant pul-
interaction monary embolism. Chest, 121[3],
• Septal shift 877–905.)
• Pericardial restriction
Decreased
CO/MAP
Decreased LV distensibility
Decreased LV preload
Medical Management PE. Although the time and costs involved with the invasive pul-
The diagnosis of PE is challenging, because PE can mimic other monary angiography preclude its routine use in the diagnosis of
cardiorespiratory or musculoskeletal disorders such as myocardial PE, it remains the most reliable clinical study available. 17 Recent
infarction, pneumonia, congestive heart failure, asthma, or costo- radiological advances now include the spiral chest computed to-
chondritis. The diagnosis of PE should always be confirmed by mography (CT), which is a newer test used in diagnosing PE. The
objective tests. However, there are few tests that are specific for strength of the spiral CT is its ability to detect emboli in the cen-
PE. Because the protective mechanism of fibrinolysis is triggered tral arteries but it is not as sensitive for finding peripheral emboli
with the formation of a clot, tests reflecting fibrinolysis have been in the pulmonary vasculature. 20 Both tests require a significant
helpful in making the diagnosis of PE. The quantitative plasma contrast dye load and this fact should be considered when decid-
D-dimer enzyme-linked immunosorbent assay (ELISA) level is el- ing on the test. Contrast-induced nephropathy may be caused by
evated ( 500 ng/mL) in more than 90% of patients with PE but direct toxic effects on the tubular epithelial cells by the formation
is not specific and therefore not useful when considering hospital- of reactive oxygen species or reduced antioxidant activity. 27 De-
ized patients. 26 ABG values are not valuable in the diagnosis of creased renal function from contrast dye load may also be caused
PE, which is contrary to classic teaching. The expected hypoxemia by an alteration in renal hemodynamics resulting in renal vaso-
associated with PE was not found to be consistently present in pa- constriction and erythrocyte aggregation. 27 The hallmark inter-
tients with documented PE. The ECG may be abnormal with an vention for prevention of contrast-induced nephropathy is hydra-
S wave in lead I, a Q wave in lead III, and inverted T wave in lead tion, usually with normal saline. 27 Hydration with sodium
III; however, these changes are usually seen in patients with a mas- bicarbonate has also been shown to be as effective as hydration
sive PE. A normal chest radiograph in a dyspneic patient could with normal saline. 11 Administration of acetylcysteine before and
suggest a possible PE. 26 However, a more definitive diagnosis can after dye load has been shown to have renal vasodilatory effects as
be made by means of a noninvasive lung VQ scan. In PE, a defect well as antioxidant benefits. 28 However, a meta-analysis did not
is evident in the perfusion portion of the scan in conjunction with clearly confirm the efficacy of acetylcysteine. 27
a normal ventilation scan. An abnormal VQ scan suggests PE. If Once PE is diagnosed, anticoagulation is the first intervention.
the VQ scan is normal, the likelihood of PE is low. This test needs The previous section on anticoagulation for DVT discusses the
to be carefully evaluated since pre-existing cardiopulmonary dis- usual approach for treatment. If the patient is severely compro-
ease can distort the interpretation and both the ventilation and mised and experiencing cardiopulmonary failure due to a PE,
perfusion portion of the test should be performed. thrombolytic therapy is indicated. Caval interruption or inferior
If the VQ scan is nondiagnostic, a pulmonary angiogram should vena cava filter can also be used to treat a PE. This intervention
be performed and is considered the gold standard. A definitive di- helps prevent passage of emboli to the lung and is used in cases
agnosis of PE is best made by pulmonary angiography because a where anticoagulation may not be appropriate. There are two
well-performed pulmonary angiogram excludes the diagnosis of types of filters: bird’s nest filter, which is placed infrarenally, and