
Page 748 - Cardiac Nursing
P. 748
009
9/2
1 A
8:3
9/0
37.
37.
0
qxd
24
24
ara
Apt
e 7
P
M
g
P
2-7
K34
0-c
30_
K34
LWB K34 0-c 30_ p72 2-7 37. qxd 0 9/0 9/2 009 0 0 8:3 1 A M P a a g e 7 24 Apt ara
L L LWB
LWBK340-c30_30_p722-737.qxd 09/09/2009 08:31 AM Page 724 Aptara
p72
724 PA R T I V / Pathophysiology and Management of Heart Disease
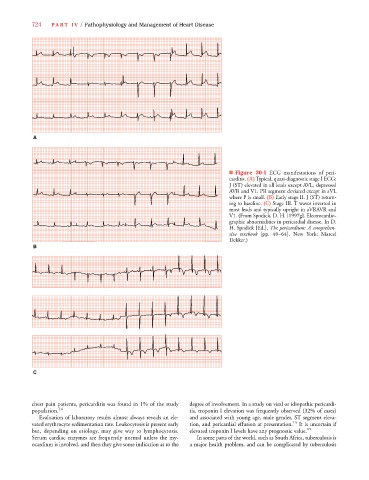
■ Figure 30-1 ECG manifestations of peri-
carditis. (A) Typical, quasi-diagnostic stage I ECG:
J (ST) elevated in all leads except AVL, depressed
AVR and V1. PR segment deviated except in aVL
where P is small. (B) Early stage II. J (ST) return-
ing to baseline. (C) Stage III. T waves inverted in
most leads and typically upright in aVRAVR and
V1. (From Spodick, D. H. [1997g]. Electrocardio-
graphic abnormalities in pericardial disease. In D.
H. Spodick [Ed.], The pericardium: A comprehen-
sive textbook [pp. 40–64]. New York: Marcel
Dekker.)
B
C
chest pain patients, pericarditis was found in 1% of the study degree of involvement. In a study on viral or idiopathic pericardi-
population. 14 tis, troponin I elevation was frequently observed (32% of cases)
Evaluation of laboratory results almost always reveals an ele- and associated with young age, male gender, ST segment eleva-
vated erythrocyte sedimentation rate. Leukocytosis is present early tion, and pericardial effusion at presentation. 15 It is uncertain if
but, depending on etiology, may give way to lymphocytosis. elevated troponin I levels have any prognostic value. 15
Serum cardiac enzymes are frequently normal unless the my- In some parts of the world, such as South Africa, tuberculosis is
ocardium is involved, and then they give some indication as to the a major health problem, and can be complicated by tuberculosis