
Page 264 - ACCCN's Critical Care Nursing
P. 264
Cardiovascular Alterations and Management 241
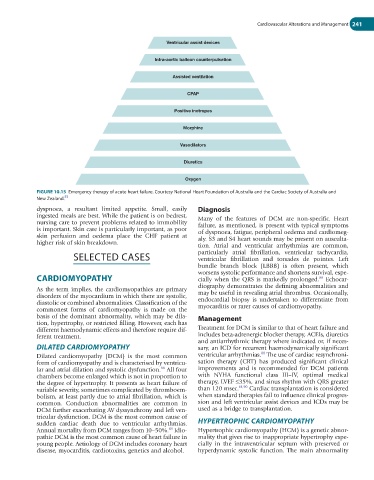
Ventricular assist devices
Intra-aortic balloon counterpulsation
Assisted ventilation
CPAP
Positive inotropes
Morphine
Vasodilators
Diuretics
Oxygen
FIGURE 10.15 Emergency therapy of acute heart failure. Courtesy National Heart Foundation of Australia and the Cardiac Society of Australia and
55
New Zealand.
dyspnoea, a resultant limited appetite. Small, easily Diagnosis
ingested meals are best. While the patient is on bedrest, Many of the features of DCM are non-specific. Heart
nursing care to prevent problems related to immobility failure, as mentioned, is present with typical symptoms
is important. Skin care is particularly important, as poor of dyspnoea, fatigue, peripheral oedema and cardiomeg-
skin perfusion and oedema place the CHF patient at aly. S3 and S4 heart sounds may be present on ausculta-
higher risk of skin breakdown.
tion. Atrial and ventricular arrhythmias are common,
SELECTED CASES particularly atrial fibrillation, ventricular tachycardia,
ventricular fibrillation and torsades de pointes. Left
bundle branch block (LBBB) is often present, which
worsens systolic performance and shortens survival, espe-
CARDIOMYOPATHY cially when the QRS is markedly prolonged. Echocar-
88
diography demonstrates the defining abnormalities and
As the term implies, the cardiomyopathies are primary
disorders of the myocardium in which there are systolic, may be useful in revealing atrial thrombus. Occasionally,
diastolic or combined abnormalities. Classification of the endocardial biopsy is undertaken to differentiate from
commonest forms of cardiomyopathy is made on the myocarditis or rarer causes of cardiomyopathy.
basis of the dominant abnormality, which may be dila- Management
tion, hypertrophy, or restricted filling. However, each has
different haemodynamic effects and therefore require dif- Treatment for DCM is similar to that of heart failure and
ferent treatment. includes beta-adrenergic blocker therapy, ACEIs, diuretics
and antiarrhythmic therapy where indicated or, if neces-
DILATED CARDIOMYOPATHY sary, an ICD for recurrent haemodynamically significant
88
Dilated cardiomyopathy (DCM) is the most common ventricular arrhythmias. The use of cardiac resynchroni-
form of cardiomyopathy and is characterised by ventricu- sation therapy (CRT) has produced significant clinical
lar and atrial dilation and systolic dysfunction. All four improvements and is recommended for DCM patients
88
chambers become enlarged which is not in proportion to with NYHA functional class III–IV, optimal medical
the degree of hypertrophy. It presents as heart failure of therapy, LVEF ≤35%, and sinus rhythm with QRS greater
variable severity, sometimes complicated by thromboem- than 120 msec. 61,90 Cardiac transplantation is considered
bolism, at least partly due to atrial fibrillation, which is when standard therapies fail to influence clinical progres-
common. Conduction abnormalities are common in sion and left ventricular assist devices and ICDs may be
DCM further exacerbating AV dyssynchrony and left ven- used as a bridge to transplantation.
tricular dysfunction. DCM is the most common cause of
sudden cardiac death due to ventricular arrhythmias. HYPERTROPHIC CARDIOMYOPATHY
Annual mortality from DCM ranges from 10–50%. Idio- Hypertrophic cardiomyopathy (HCM) is a genetic abnor-
89
pathic DCM is the most common cause of heart failure in mality that gives rise to inappropriate hypertrophy espe-
young people. Aetiology of DCM includes coronary heart cially in the intraventricular septum with preserved or
disease, myocarditis, cardiotoxins, genetics and alcohol. hyperdynamic systolic function. The main abnormality