
Page 2616 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 2616
Chapter 161 Hematology in Aging 2329
TABLE Anemia Definitions TABLE Hematopoietic Changes Associated With Advancing
161.1 161.2 Age
Group Hemoglobin (g/dL) Diminished bone marrow cellularity
+
Men, 60 Years or Older Reduced CD34 cell mobilization to G-CSF administration in healthy
White 13.2 donors
Decreased stem cell telomeres
Black 12.7 Reduced hematopoietic cell proliferative capacity
Women, 50 Years or Older Increased numbers of hematopoietic stem cells
White 12.2 Reduction in lymphocyte function
Black 11.5 Reduced response to vaccination
Development of unexplained anemia
Adapted from Beutler E, Waalen J: The definition of anemia: what is the lower
limit of normal of the blood hemoglobin concentration? Blood 107:1747, 2006. G-CSF, Granulocyte colony-stimulating factor.
Prevalence of Anemia by Category Evaluating Anemia in Older Adults
Anemia in older adults is a common finding and frequently results in
5.7% a request for hematology consultation.
4.6% To define anemia, we apply the Beutler and Waalen criteria in Table
3.4% 161.1 but also evaluate hemoglobin trajectories over time based on
remote laboratory values when available. Based on the fact that the
average hemoglobin level declines in older adults about 1 g/dL over 15
7.5% 19
years or more, we consider a decline of 1 g/dL in less than 5 years
44% or 2 g/dL over 10 years significant, and this also supports the need to
pursue a complete evaluation.
9.8% To elicit symptoms, both the patient and family members and
caregivers are asked about functional changes (walking, naps, activity
level) and the duration (weeks, months or years). Because the etiology
of anemia can be multifactorial, we routinely perform the same panel
25% on most patients: complete blood count, white blood cell differential,
red blood cell indices, reticulocyte count, smear review, serum fer-
ritin, serum iron, total iron-binding capacity, serum creatinine (and
estimated renal function), vitamin B 12, and thyrotropin levels. Mean
corpuscular volume is helpful but imperfect. We also have found high
C-reactive protein (i.e., >10 mg/L) consistent with an inflammatory
UAE CKD
process and high serum erythropoietin (above the reference range)
IDA Thal suspicious for iron deficiency, hematologic malignancy, or hyperpro-
ACI Oth ductive anemias. Folate levels are rarely useful in countries practicing
Heme Malig universal dietary supplementation. The remainder of the laboratory
tests will be performed as indicated.
A ferritin level of less than 50 ng/mL prompts a complete evaluation
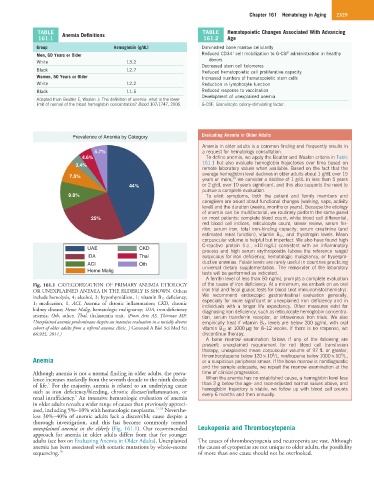
Fig. 161.1 CATEGORIZATION OF PRIMARY ANEMIA ETIOLOGY of the cause of iron deficiency. At a minimum, we embark on an oral
OR UNEXPLAINED ANEMIA IN THE ELDERLY IS SHOWN. Others iron trial and fecal guaiac tests for blood (not immunohistochemistry).
include hemolysis, 4; alcohol, 3; hypothyroidism, 1; vitamin B 12 deficiency, We recommend endoscopic gastrointestinal evaluation generally,
1; medication, 1. ACI, Anemia of chronic inflammation; CKD, chronic especially for more significant or unexplained iron deficiency and in
individuals with a longer life expectancy. Other measures exist for
kidney disease; Heme Malig, hematologic malignancy; IDA, iron-deficiency diagnosing iron deficiency, such as reticulocyte hemoglobin concentra-
anemia; Oth, other; Thal, thalassemia trait. (From Artz AS, Thirman MF: tion, serum transferrin receptor, or intravenous iron trials. We also
Unexplained anemia predominates despite an intensive evaluation in a racially diverse empirically treat if vitamin B 12 levels are below 200 pg/mL with oral
cohort of older adults from a referral anemia clinic. J Gerontol A Biol Sci Med Sci vitamin B 12 at 1000 µg for 8–12 weeks. If there is no response, we
66:925, 2011.) discontinue therapy.
A bone marrow examination follows if any of the following are
present: unexplained requirement for red blood cell transfusion
therapy, unexplained mean corpuscular volume of 97 fL or greater,
9
9
thrombocytopenia below 120 × 10 /L, neutropenia below 1000 × 10 /L,
Anemia or a suspicious peripheral smear. If the bone marrow is nondiagnostic
and the sample adequate, we repeat the marrow examination at the
Although anemia is not a normal finding in older adults, the preva- time of clinical progression.
lence increases markedly from the seventh decade to the ninth decade When the anemia has no established cause, a hemoglobin level less
5
of life. For the majority, anemia is related to an underlying cause than 2 g below the age- and race-adjusted normal values above, and
such as iron deficiency/bleeding, chronic disease/inflammation, or hemoglobin trajectory is stable, we follow up with blood cell counts
every 6 months and then annually.
5
renal insufficiency. An intensive hematologic evaluation of anemia
in older adults reveals a wider range of causes than previously appreci-
ated, including 5%–10% with hematologic neoplasms. 17,18 Neverthe-
less 30%–40% of anemic adults lack a discernible cause despite a
thorough investigation, and this has become commonly termed
unexplained anemia in the elderly (Fig. 161.1). Our recommended Leukopenia and Thrombocytopenia
approach for anemia in older adults differs from that for younger
adults (see box on Evaluating Anemia in Older Adults). Unexplained The causes of thrombocytopenia and neutropenia are vast. Although
anemia has been associated with somatic mutations by whole-exome the causes of cytopenias are not unique to older adults, the possibility
sequencing. 16 of more than one cause should not be overlooked.