
Page 736 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 736
Chapter 44 Red Blood Cell Enzymopathies 623
O 2
2+
Fe deoxyhemoglobin
2+
Fe oxyhemoglobin
NAD NADP
b5R Methylene blue
ROS
NADH NADPH
Endogenous and
exogenous ROS Treatment of acute
methemoglobinemia
3+
Fe methemoglobin
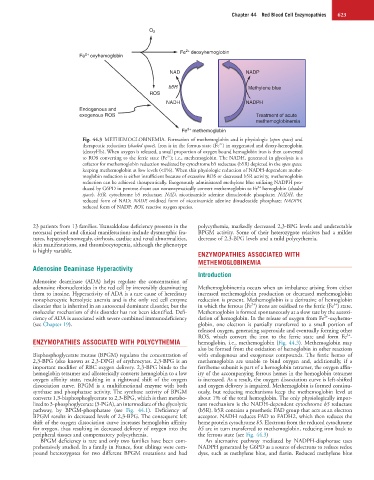
Fig. 44.3 METHEMOGLOBINEMIA. Formation of methemoglobin and it physiologic (open space) and
2+
therapeutic reduction (shaded space). Iron is in the ferrous state (Fe ) in oxygenated and deoxy-hemoglobin
(deoxyHb). When oxygen is released, a small proportion of oxygen bound hemoglobin iron is then converted
3+
to ROS converting to the ferric state (Fe ); i.e., methemoglobin. The NADH, generated in glycolysis is a
cofactor for methemoglobin reduction mediated by cytochrome b5 reductase (b5R) depicted in the open space,
keeping methemoglobin at low levels (<1%). When this physiologic reduction of NADH-dependent methe-
moglobin reduction is either insufficient because of excessive ROS or decreased b5R activity, methemoglobin
reduction can be achieved therapeutically. Exogenously administered methylene blue utilizing NADPH pro-
2+
duced by G6PD in pentose shunt can nonenzymatically convert methemoglobin to Fe hemoglobin (shaded
space). b5R, cytochrome b5 reductase; NAD, nicotinamide adenine dinucleotide phosphate; NADH, the
reduced form of NAD; NADP, oxidized form of nicotinamide adenine dinucleotide phosphate; NADPH,
reduced form of NADP; ROS, reactive oxygen species.
23 patients from 13 families. Transaldolase deficiency presents in the polycythemia, markedly decreased 2,3-BPG levels and undetectable
neonatal period and clinical manifestations include dysmorphic fea- BPGM activity. Some of their heterozygote relatives had a milder
tures, hepatosplenomegaly, cirrhosis, cardiac and renal abnormalities, decrease of 2,3-BPG levels and a mild polycythemia.
skin manifestations, and thrombocytopenia, although the phenotype
is highly variable.
ENZYMOPATHIES ASSOCIATED WITH
METHEMOGLOBINEMIA
Adenosine Deaminase Hyperactivity
Introduction
Adenosine deaminase (ADA) helps regulate the concentration of
adenosine ribonucleotides in the red cell by irreversibly deaminating Methemoglobinemia occurs when an imbalance arising from either
them to inosine. Hyperactivity of ADA is a rare cause of hereditary increased methemoglobin production or decreased methemoglobin
nonspherocytic hemolytic anemia and is the only red cell enzyme reduction is present. Methemoglobin is a derivative of hemoglobin
2+
3+
disorder that is inherited in an autosomal dominant disorder, but the in which the ferrous (Fe ) irons are oxidized to the ferric (Fe ) state.
molecular mechanism of this disorder has not been identified. Defi- Methemoglobin is formed spontaneously at a slow rate by the autoxi-
2+
ciency of ADA is associated with severe combined immunodeficiency dation of hemoglobin. In the release of oxygen from Fe -oxyhemo-
(see Chapter 19). globin, one electron is partially transferred to a small portion of
released oxygen, generating superoxide and eventually forming other
3+
ROS, which convert the iron to the ferric state and form Fe -
ENZYMOPATHIES ASSOCIATED WITH POLYCYTHEMIA hemoglobin, i.e., methemoglobin (Fig. 44.3). Methemoglobin may
also be formed from the oxidation of hemoglobin in other reactions
Bisphosphoglycerate mutase (BPGM) regulates the concentration of with endogenous and exogenous compounds. The ferric hemes of
2,3-BPG (also known as 2,3-DPG) of erythrocytes. 2,3-BPG is an methemoglobin are unable to bind oxygen and, additionally, if a
important modifier of RBC oxygen delivery. 2,3-BPG binds to the ferriheme subunit is part of a hemoglobin tetramer, the oxygen affin-
hemoglobin tetramer and allosterically converts hemoglobin to a low ity of the accompanying ferrous hemes in the hemoglobin tetramer
oxygen affinity state, resulting in a rightward shift of the oxygen is increased. As a result, the oxygen dissociation curve is left-shifted
dissociation curve. BPGM is a multifunctional enzyme with both and oxygen delivery is impaired. Methemoglobin is formed continu-
synthase and phosphatase activity. The synthase activity of BPGM ously, but reducing mechanisms keep the methemoglobin level at
converts 1,3-bisphosphoglycerate to 2,3-BPG, which is then metabo- about 1% of the total hemoglobin. The only physiologically impor-
lized to 3-phosphoglycerate (3-PGA), an intermediate of the glycolytic tant mechanism is the NADH-dependent cytochrome b5 reductase
pathway, by BPGM-phosphatase (see Fig. 44.1). Deficiency of (b5R). b5R contains a prosthetic FAD group that acts as an electron
BPGM results in decreased levels of 2,3-BPG. The consequent left acceptor. NADH reduces FAD to FADH2, which then reduces the
shift of the oxygen dissociation curve increases hemoglobin affinity heme protein cytochrome b5. Electrons from the reduced cytochrome
for oxygen, thus resulting in decreased delivery of oxygen into the b5 are in turn transferred to methemoglobin, reducing iron back to
peripheral tissues and compensatory polycythemia. the ferrous state (see Fig. 44.3)
BPGM deficiency is rare and only two families have been com- An alternative pathway mediated by NADPH-diaphorase uses
prehensively studied. In a family in France, four siblings were com- NADPH generated by G6PD as a source of electrons to reduce redox
pound heterozygotes for two different BPGM mutations and had dyes, such as methylene blue, and flavin. Reduced methylene blue