
Page 2065 - Williams Hematology ( PDFDrive )
P. 2065
2040 Part XII: Hemostasis and Thrombosis Chapter 120: Hereditary Qualitative Platelet Disorders 2041
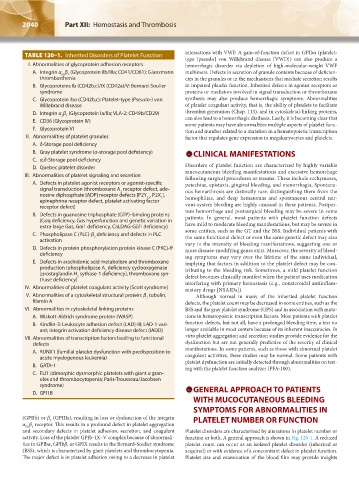
TABLE 120–1. Inherited Disorders of Platelet Function interactions with VWF. A gain-of-function defect in GPIbα (platelet-
type [pseudo] von Willebrand disease [VWD]) can also produce a
I. Abnormalities of glycoprotein adhesion receptors hemorrhagic disorder via depletion of high-molecular-weight VWF
A. Integrin α β (Glycoprotein IIb/IIIa; CD41/CD61): Glanzmann multimers. Defects in secretion of granule contents because of deficien-
IIb 3
thrombasthenia cies in the granules or in the mechanisms that mediate secretion results
B. Glycoproteins Ib (CD42b,c)/IX (CD42a)/V: Bernard-Soulier in impaired platelet function. Inherited defects in agonist receptors or
syndrome proteins or mediators involved in signal transduction or thromboxane
C. Glycoprotein Ibα (CD42b,c): Platelet-type (Pseudo-) von synthesis may also produce hemorrhagic symptoms. Abnormalities
Willebrand disease of platelet coagulant activity, that is, the ability of platelets to facilitate
D. Integrin α β (Glycoprotein Ia/IIa; VLA-2; CD49b/CD29) thrombin generation (Chap. 113), and in cytoskeletal-linking proteins,
2 1 can also lead to a hemorrhagic diathesis. Lastly, it is becoming clear that
E. CD36 (Glycoprotein IV) some patients may have abnormalities multiple aspects of platelet func-
F. Glycoprotein VI tion and number related to a mutation in a hematopoietic transcription
II. Abnormalities of platelet granules factor that regulates gene expression in megakaryocytes and platelets.
A. δ-Storage pool deficiency
B. Gray platelet syndrome (α-storage pool deficiency) CLINICAL MANIFESTATIONS
C. α,δ-Storage pool deficiency
D. Quebec platelet disorder Disorders of platelet function are characterized by highly variable
III. Abnormalities of platelet signaling and secretion mucocutaneous bleeding manifestations and excessive hemorrhage
following surgical procedures or trauma. These include ecchymoses,
A. Defects in platelet agonist receptors or agonist-specific petechiae, epistaxis, gingival bleeding, and menorrhagia. Spontane-
signal transduction (thromboxane A receptor defect, ade- ous hemarthrosis are distinctly rare, distinguishing them from the
2
nosine diphosphate [ADP] receptor defects [P2Y , P2X ], hemophilias, and deep hematomas and spontaneous central ner-
12
1
epinephrine receptor defect, platelet activating factor
receptor defect) vous system bleeding are highly unusual in these patients. Postpar-
B. Defects in guanosine triphosphate (GTP)–binding proteins tum hemorrhage and postsurgical bleeding may be severe in some
patients. In general, most patients with platelet function defects
(Gαq deficiency, Gαs hyperfunction and genetic variation in
extra-large Gαs, Gαi1 deficiency, CaLDAG-GEFI deficiency) have mild to moderate bleeding manifestations, but may be severe in
C. Phospholipase C (PLC)-β deficiency and defects in PLC some entities, such as the GT and the BSS. Individual patients with
the same functional defect or even the same genetic defect may also
2
activation vary in the intensity of bleeding manifestations, suggesting one or
D. Defects in protein phosphorylation protein kinase C (PKC)-θ more disease-modifying genes exist. Moreover, the severity of bleed-
deficiency ing symptoms may vary over the lifetime of the same individual,
E. Defects in arachidonic acid metabolism and thromboxane implying that factors in addition to the platelet defect may be con-
production (phospholipase A deficiency cyclooxygenase tributing to the bleeding risk. Sometimes, a mild platelet function
2
[prostaglandin H sythase-1 deficiency], thromboxane syn- defect becomes clinically manifest when the patient uses medication
2
thase deficiency) interfering with primary hemostasis (e.g., nonsteroidal antiinflam-
IV. Abnormalities of platelet coagulant activity (Scott syndrome) matory drugs [NSAIDs]).
V. Abnormalities of a cytoskeletal structural protein: β tubulin, Although normal in many of the inherited platelet function
1
filamin A defects, the platelet count may be decreased in some entities, such as the
VI. Abnormalities in cytoskeletal linking proteins BSS and the gray platelet syndrome (GPS) and in association with muta-
A. Wiskott-Aldrich syndrome protein (WASP) tions in hematopoietic transcription factors. Most patients with platelet
B. Kindlin-3: Leukocyte adhesion defect (LAD)-III; LAD-1 vari- function defects, but not all, have a prolonged bleeding time, a test no
ant; integrin activation deficiency disease defect (IADD) longer available in most centers because of its inherent inaccuracies. In
VII. Abnormalities of transcription factors leading to functional vitro platelet aggregation and secretion studies provide evidence for the
defects dysfunction but are not generally predictive of the severity of clinical
A. RUNX1 (familial platelet dysfunction with predisposition to manifestations. In some patients, such as those with abnormal platelet
acute myelogenous leukemia) coagulant activities, these studies may be normal. Some patients with
B. GATA-1 platelet dysfunction are initially detected through abnormalities on test-
ing with the platelet function analyzer (PFA-100).
C. FLI1 (dimorphic dysmorphic platelets with giant α gran-
ules and thrombocytopenia; Paris-Trousseau/Jacobsen
syndrome)
D. GFI1B GENERAL APPROACH TO PATIENTS
WITH MUCOCUTANEOUS BLEEDING
SYMPTOMS FOR ABNORMALITIES IN
(GPIIb) or β (GPIIIa), resulting in loss or dysfunction of the integrin PLATELET NUMBER OR FUNCTION
3
α β receptor. This results in a profound defect in platelet aggregation
IIb 3
and secondary defects in platelet adhesion, secretion, and coagulant Platelet disorders are characterized by alterations in platelet number or
activity. Loss of the platelet GPIb–IX–V complex because of abnormali- function or both. A general approach is shown in Fig. 120-1. A reduced
ties in GPIbα, GPIbβ, or GPIX results in the Bernard-Soulier syndrome platelet count can occur as an isolated platelet disorder (inherited or
(BSS), which is characterized by giant platelets and thrombocytopenia. acquired) or with evidence of a concomitant defect in platelet function.
The major defect is in platelet adhesion owing to a decrease in platelet Platelet size and examination of the blood film may provide insights
Kaushansky_chapter 120_p2039-2072.indd 2040 9/21/15 2:20 PM