
Page 589 - Williams Hematology ( PDFDrive )
P. 589
564 Part VI: The Erythrocyte Chapter 39: The Congenital Dyserythropoietic Anemias 565
Primitive Committed Lineage-
progenitor cells precursor cells committed cells
Multipotent
hematopoietic
stem cell
Common myeloid FA; DKC
progenitor
*
XLTDA; DBA CDA
Myeloid erythroid CEP; XLTT
progenitor * *
*
BFU-E CFU-E Proerythroblast Basophilic Polychromatic Orthochromatic Reticulocyte Erythrocyte
A erythroblast erythroblast erythroblast
Hemolytic anemia with
inadequate reticulocyte BMF Syndromes
count
Trilineage Isolated ineffective CDA I • EM: “swiss cheese appearance” of
ineffective hematopoiesis erythropoiesis Incompletely divided cells; thin the erythroblasts heterochromatin
chromatin bridges between nuclei • Molecular diagnosis: CDAN1;
of pairs of erythroblasts C15orf41
BM examination
• EM: double plasma membrane of
CDA II the erythroblasts
Binucleate and rarely • Biochemical diagnosis: band 3
FA, AA, DKC, PNH, MDS Erythroid Erythroid multinucleate late polychromatic hypoglycosylation
hypoplasia hyperplasia erythroblasts • WB: ER proteins on RBC plasma
membrane
• Molecular diagnosis: SEC23B
CDA III
DBA Large multinucleated • Molecular diagnosis: KIF23
erythroblasts (gigantoblasts)
• Ineffective erythropoiesis; HPFH
• Molecular diagnosis: KLF1
Dyserythropoietic morphology
variants
• Ineffective megakaryopoiesis and
erythropoiesis
• Molecular diagnosis: GATA1
B
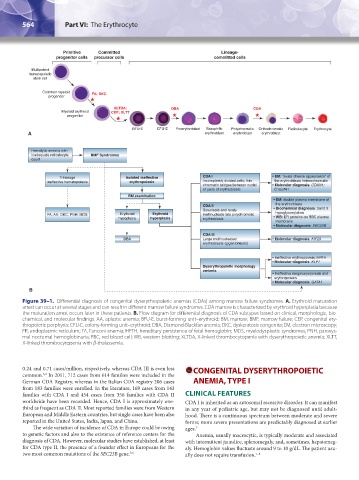
Figure 39–1. Differential diagnosis of congenital dyserythropoietic anemias (CDAs) among marrow failure syndromes. A. Erythroid maturation
arrest can occur at several stages and can result in different marrow failure syndromes. CDA marrow is characterized by erythroid hyperplasia because
the maturation arrest occurs later in these patients. B. Flow diagram for differential diagnosis of CDA subtypes based on clinical, morphologic, bio-
chemical, and molecular findings. AA, aplastic anemia; BFU-E, burst-forming unit–erythroid; BM, marrow; BMF, marrow failure; CEP, congenital ery-
thropoietic porphyria; CFU-E, colony-forming unit–erythroid; DBA, Diamond-Blackfan anemia; DKC, dyskeratosis congenita; EM, electron microscopy;
ER, endoplasmic reticulum; FA, Fanconi anemia; HPFH, hereditary persistence of fetal hemoglobin; MDS, myelodysplastic syndromes; PNH, paroxys-
mal nocturnal hemoglobinuria; RBC, red blood cell; WB, western blotting; XLTDA, X-linked thrombocytopenia with dyserythropoietic anemia; XLTT,
X-linked thrombocytopenia with β-thalassemia.
0.24 and 0.71 cases/million, respectively, whereas CDA III is even less CONGENITAL DYSERYTHROPOIETIC
common. In 2011, 712 cases from 614 families were included in the
3,4
German CDA Registry, whereas in the Italian CDA registry 206 cases ANEMIA, TYPE I
from 183 families were enrolled. In the literature, 169 cases from 143
families with CDA I and 454 cases from 356 families with CDA II CLINICAL FEATURES
worldwide have been recorded. Hence, CDA I is approximately one- CDA I is inherited as an autosomal recessive disorder. It can manifest
third as frequent as CDA II. Most reported families were from Western in any year of pediatric age, but may not be diagnosed until adult-
European and Middle Eastern countries, but single cases have been also hood. There is a continuous spectrum between moderate and severe
reported in the United States, India, Japan, and China. forms; more severe presentations are predictably diagnosed at earlier
The wide variation of incidence of CDA in Europe could be owing ages. 7
to genetic factors and also to the existence of reference centers for the Anemia, usually macrocytic, is typically moderate and associated
diagnosis of CDA. However, molecular studies have established, at least with intermittent jaundice, splenomegaly, and, sometimes, hepatomeg-
for CDA type II, the presence of a founder effect in Europeans for the aly. Hemoglobin values fluctuate around 9 to 10 g/dL. The patient usu-
two most common mutations of the SEC23B gene. 5,6 ally does not require transfusion. 7–9
Kaushansky_chapter 39_p0563-0570.indd 564 9/17/15 6:21 PM