
Page 494 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 494
474 PARt fouR Immunological Deficiencies
TABLE 34.2 Laboratory Diagnosis of Primary Antibody Deficiency
Level test Application(s)
I CBC with differential Primary screening tests
Complement (CH 50 , C3, C4, mannose-binding lectin [MBL] protein)
Erythrocyte sedimentation rate (ESR)
Quantitative serum immunoglobulin (Ig)M, IgG, and IgA levels
Ia Urinalysis, 24-hour urine for protein Symptoms suggest protein loss
Stool for α-1-antitrypsin through kidneys or
gastrointestinal (GI) tract
II B-cell functional evaluation Level I normal but history suggests
Quantitative IgG subclasses, IgE Antibody deficiency
Natural or commonly acquired antibodies (isohemagglutinins, rubella, rubeola, tetanus) Better definition of a level I defect
Response to immunization
T cell–dependent antigens (tetanus)
T cell–independent antigens (unconjugated pneumococcal vaccine, unconjugated H. influenzae
B vaccine)
III Quantification of blood T-and B-cell subpopulations by immunofluorescence assays using Panhypogammaglobulinemia or
monoclonal antibody markers severely low IgM and IgA
T cells: CD3, CD4, CD8
B cells: CD19, CD20, CD21, Ig (µ, δ, κ, λ),
IV Disease-specific analysis Gene-specific diagnosis
Gene expression Genetic counseling
Gene sequencing
1300
IgG
1100 Maternal IgG
Average serum immunoglobulin concentration (mg/dL) 500 Child’s IgG IgA
900
700
300
250
200
150
100
50 IgM
25
0
0 2 4 6 8 2 4 6 810122 4 6 810 1525351255657585
Months Birth Months Years
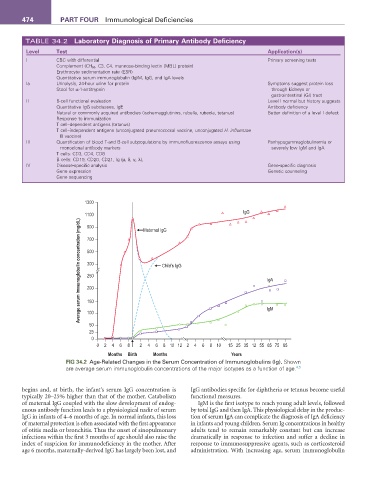
fIG 34.2 Age-Related Changes in the Serum Concentration of Immunoglobulins (Ig). Shown
4,5
are average serum immunoglobulin concentrations of the major isotypes as a function of age.
begins and, at birth, the infant’s serum IgG concentration is IgG antibodies specific for diphtheria or tetanus become useful
typically 20–25% higher than that of the mother. Catabolism functional measures.
of maternal IgG coupled with the slow development of endog- IgM is the first isotype to reach young adult levels, followed
enous antibody function leads to a physiological nadir of serum by total IgG and then IgA. This physiological delay in the produc-
IgG in infants of 4–6 months of age. In normal infants, this loss tion of serum IgA can complicate the diagnosis of IgA deficiency
of maternal protection is often associated with the first appearance in infants and young children. Serum Ig concentrations in healthy
of otitis media or bronchitis. Thus the onset of sinopulmonary adults tend to remain remarkably constant but can increase
infections within the first 3 months of age should also raise the dramatically in response to infection and suffer a decline in
index of suspicion for immunodeficiency in the mother. After response to immunosuppressive agents, such as corticosteroid
age 6 months, maternally-derived IgG has largely been lost, and administration. With increasing age, serum immunoglobulin