
Page 1128 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1128
CHAPTER 83: ICU-Acquired Weakness 767
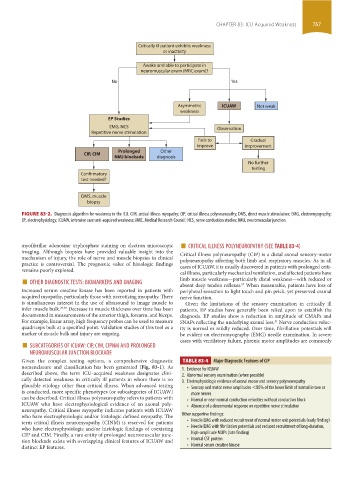
Critically ill patient exhibits weakness
or inactivity
Awake and able to participate in
neuromuscular exam (MRC exam)?
No Yes
Asymmetric ICUAW Not weak
weakness
EP Studies
EMG, NCS Observation
Repetitive nerve stimulation
Fails to Gradual
improve improvement
Prolonged Other
CIP, CIM
NMJ blockade diagnosis
No further
testing
Confirmatory
test needed?
DMS, muscle
biopsy
FIGURE 83-2. Diagnostic algorithm for weakness in the ICU. CIM, critical illness myopathy; CIP, critical illness polyneuropathy; DMS, direct muscle stimulation; EMG, electromyography;
EP, electrophysiology; ICUAW, intensive care unit-acquired weakness; MRC, Medical Research Council; NCS, nerve conduction studies; NMJ, neuromuscular junction.
■
myofibrillar adenosine triphosphate staining on electron microscopic CRITICAL ILLNESS POLYNEUROPATHY (SEE TABlE 83-4)
imaging. Although biopsies have provided valuable insight into the Critical illness polyneuropathy (CIP) is a distal axonal sensory-motor
mechanism of injury, the role of nerve and muscle biopsies in clinical polyneuropathy affecting both limb and respiratory muscles. As in all
practice is controversial. The prognostic value of histologic findings cases of ICUAW, it is usually discovered in patients with prolonged criti-
remains poorly explored. cal illness, particularly mechanical ventilation, and affected patients have
■ OTHER DIAGNOSTIC TESTS: BIOMARKERS AND IMAGING limb muscle weakness—particularly distal weakness—with reduced or
27
Increased serum creatine kinase has been reported in patients with absent deep tendon reflexes. When measurable, patients have loss of
peripheral sensation to light touch and pin prick, yet preserved cranial
acquired myopathy, particularly those with necrotizing myopathy. There nerve function.
is simultaneous interest in the use of ultrasound to image muscle to Given the limitations of the sensory examination in critically ill
infer muscle bulk. 29,30 Decrease in muscle thickness over time has been patients, EP studies have generally been relied upon to establish the
documented in measurements of the anterior thigh, forearm, and biceps. diagnosis. EP studies show a reduction in amplitude of CMAPs and
For example, linear array, high frequency probes can be used to measure SNAPs reflecting the underlying axonal loss. Nerve conduction veloc-
31
quadriceps bulk at a specified point. Validation studies of this tool as a ity is normal or mildly reduced. Over time, fibrillation potentials will
marker of muscle bulk and injury are ongoing. be evident on electromyography (EMG) needle examination. In severe
■ SUBCATEGORIES OF ICUAW: CIP, CIM, CIPNM AND PROLONGED cases with ventilatory failure, phrenic motor amplitudes are commonly
NEUROMUSCULAR JUNCTION BLOCKADE
Given the complex testing options, a comprehensive diagnostic TABLE 83-4 Major Diagnostic Features of CIP
nomenclature and classification has been generated (Fig. 83-1). As 1. Evidence for ICUAW
described above, the term ICU-acquired weakness designates clini- 2. Abnormal sensory examination (when possible)
cally detected weakness in critically ill patients in whom there is no 3. Electrophysiologic evidence of axonal motor and sensory polyneuropathy
plausible etiology other than critical illness. When advanced testing • Sensory and motor nerve amplitudes <80% of the lower limit of normal in two or
is conducted, more specific phenotypes (or subcategories of ICUAW) more nerves
can be described. Critical illness polyneuropathy refers to patients with • Normal or near normal conduction velocities without conduction block
ICUAW who have electrophysiological evidence of an axonal poly- • Absence of a decremental response on repetitive nerve stimulation
neuropathy. Critical illness myopathy indicates patients with ICUAW
who have electrophysiologic and/or histologic defined myopathy. The Other supportive findings:
term critical illness neuromyopathy (CINM) is reserved for patients • Needle EMG with reduced recruitment of normal motor unit potentials (early finding)
who have electrophysiologic and/or histologic findings of coexisting • Needle EMG with fibrillation potentials and reduced recruitment of long-duration,
CIP and CIM. Finally, a rare entity of prolonged neuromuscular junc- high-amplitude MUPs (late finding)
tion blockade exists with overlapping clinical features of ICUAW and • Normal CSF protein
distinct EP features. • Normal serum creatine kinase
section06.indd 767 1/23/2015 12:55:31 PM