
Page 147 - fbkCardioDiabetes_2017
P. 147
Cardio Diabetes Medicine 2017 123
are therefore usually fasting(defined as at least 8h triglyceride levels.
since the last meal) only for few hours. For all these In another study, a readuced fructose intake signifi-
reasons,non- Fasting Lipid concentrations might be cantly lowered triglyceride levels. 30, Thus nonpharma-
a better indicator of average lipid concentrations in cologic interventions,such as weight loss in obese
the blood rather than fasting concentrations.
optients,aerobic exercise avoidance of concentrated
sugars and medications that raise serum triglyceride
Hypertriglyceridemia and serum cholesterol levels, and strict glycemic control in diabetics should
A combination of hypertriglyceridemia with hypercho- be first-line therapy. other risk factors for CV dis-
31
lesterolemia carries greater tendency to atherosclero- ease,such as hypertension and smoking should also
sis when compared to hypercholesterolemia alone. be addressed.
Small VLDL, IDL,and β-VLDL are more inherently
atherogenic 22,23 The presence of hypertriglyceridemia Alcohol abuse must be avoided in patients with ser-
suggests that increase in serum total cholesterol is vere hypertriglyceridemia as it can cause large in-
32
partially due to increased very low density lipopro- crease in triglyceride levels precipitate pancreatitis.
tein- cholesterol(VLDL-C).This relationship also has it is preferable for patients with mild – to- moderate
therapeutic implications Treatment to reduce serum hypertriglycerdemia to limit their alcohol consump-
triglyceride with nicotinic acid or fibrates will also re- tion to less than two drinks per day in men and one
duce total cholesterol. Statins have a smaller effect drink per day in women.
on VLDL compared to LDL compared to LDL,and
therefore, are weak in reducing total serum choles- Pharmacotherapy for hypertriglycerdemia:
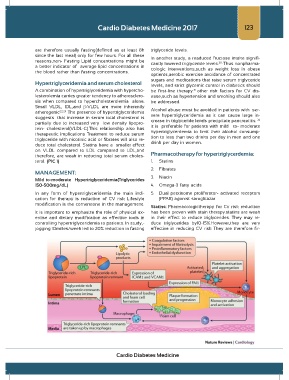
terol. (PIC 1) 1. Statins
2. Fibrates
MANAGEMENT:
Mild–to-moderate Hypertriglyceridemia(Triglycerides 3. Niacin
150-500mg/dL) 4. Omega-3 fatty acids
In any form of hypertriglyceridemia the main indi- 5. Dual perxisome proliferator- activated receptors
cation for therapy is reduction of CV risk Lifestyle (PPAR) agonist saroglitazar
modification is the cornerstone in the management.
Statins: Pharmacologictherapy for Cv risk reduction
It is important to emphasize the role of physical ex- has been proven with stain therapy.statins are weak
ercise and dietary modification as effective tools in in their effect to reduce triglycerides. They may re-
controlling hypertriglyceridemia to patients. In study,- duce triglycerides by10-15%.However,they are very
jogging 10milles/week led to 20% reduction in fasting effective in reducing CV risk They are therefore fir-
Cardio Diabetes Medicine