
Page 162 - fbkCardioDiabetes_2017
P. 162
138 Cardio Diabetes Medicine 2017
gender is observed as risk factor for neurogenic car- carboxykinase(PEPCK) and glycogen phosphory-
diac enzyme elevation. The pattern of enzyme eleva- lase (GPase) thereby resulting in hyperglycemia. In
tion in coronary artery disease and neurogenic myo- skeletal muscles, down regulation of insulin recep-
cardial injury are different, helping us to differentiate tor expression results in decreased translocation of
between the two. In case of neurogenic myocardial glucose transporter (GLUT4) into plasma membrane
damage the rate of enzyme elevation will be slow and hence hyperglycemia, because of impaired glu-
and the peak values will be low but in coronary artery cose utilization by the skeletal muscles
disease related myocardial injury there will be rapid
elevation of cardiac enzymes and the peak values
will be high .
(1)
Effects of stroke on diabetes
The effect of diabetes on the pathogenesis and the
outcome of stroke is a well known entity. But, not
much is known about the effects of stroke on diabe-
tes and more research is needed to explore this area.
Diabetes and stroke produces detrimental effects on
each other, setting a vicious cycle at least during the
acute phase of stroke. Most evidences (animal and
human) available for the effects of stroke on diabe-
tes are for ischemic strokes.
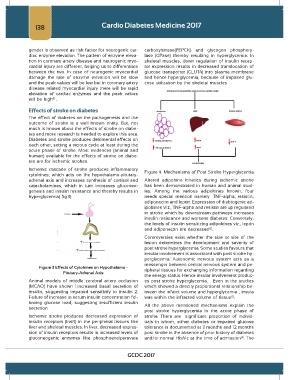
Ischemic cascade of stroke produces inflammatory Figure 4. Mechanisms of Post Stroke Hyperglycemia
cytokines, which acts on the hypothalamo-pitutary-
adrenal axis and increases synthesis of cortisol and Altered adipokine kinetics during ischemic stroke
catecholamines, which in turn increases gluconeo- has been demonstrated in human and animal stud-
genesis and insulin resistance and thereby results in ies. Among the various adipokines known, four
hyperglycemia( fig.3) needs special mention namely –TNF-alpha, resistin,
adiponectin and leptin. Expression of diabtogenic ad-
ipokines Viz., TNF-alpha and resistin are up regulated
in stroke which by downstream pathways increases
insulin resistance and worsens diabetes. Conversely,
the levels of insulin sensitizing adipokines viz., leptin
and adiponectin are decreased .
(2)
Controversies exist whether the size or site of the
lesion determines the development and severity of
post stroke hyperglycemia. Some studies favours that
insular involvement is associated with post stroke hy-
. perglycemia. Autonomic nervous system acts as a
messenger between central nervous system and pe-
Figure 3 Effects of Cytokines on Hypothalamo - ripheral tissues for exchanging information regarding
Pitutary-Adrenal Axis
the energy status. Hence insular involvement produc-
Animal models of middle cerebral artery occlusion es post stroke hyperglycemia. Even in the studies
(MCAO) have shown 1.increased basal secretion of which showed a directly proportional relationship be-
insulin, suggesting impaired sensitivity to insulin 2. tween the infarct volume and hyperglycemia , insula
(2)
Failure of increase in serum insulin concentration fol- was within the infracted volume of tissue .
lowing glucose load, suggesting insufficient insulin All the above mentioned mechanisms explain the
secretion.
post stroke hyperglycemia in the acute phase of
Ischemic stroke produces decreased expression of stroke. There are significant proportion of individ-
insulin receptors (InsR) in the peripheral tissues like uals in whom, either diabetes or impaired glucose
liver and skeletal muscles. In liver, decreased expres- tolerance is documented at 3 months and 12 months
sion of insulin receptors results in increased levels of post stroke in the absence of prior history of diabetes
gluconeogenic enzymes like phosphoenolpyruvate and/or normal HbA1c at the time of admission . The
(4)
GCDC 2017