
Page 167 - fbkCardioDiabetes_2017
P. 167
Cardio Diabetes Medicine 2017 143
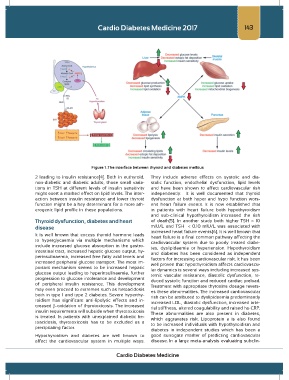
Figure 1 .The interface between thyroid and diabetes mellitus
2 leading to insulin resistance[4]. Both in euthyroid, They include adverse effects on systolic and dia-
non-diabetic and diabetic adults, those small varia- stolic function, endothelial dysfunction, lipid levels
tions in TSH at different levels of insulin sensitivity and have been shown to affect cardiovascular risk
might exert a marked effect on lipid levels. The inter- independently. It is well documented that thyroid
action between insulin resistance and lower thyroid dysfunction at both hyper and hypo function wors-
function might be a key determinant for a more ath- ens heart failure events. It is now established that
erogenic lipid profile in these populations. in patients with heart failure both hypothyroidism
and sub-clinical hypothyroidism increased the risk
Thyroid dysfunction, diabetes and heart of death[5]. In another study both higher TSH > 10
disease mIU/L and TSH < 0.10 mIU/L was associated with
It is well known that excess thyroid hormone leads increased heart failure events[6]. It is well known that
heart failure is a final common pathway affecting the
to hyperglycaemia via multiple mechanisms which cardiovascular system due to poorly treated diabe-
include increased glucose absorption in the gastro- tes, dyslipidaemia or hypertension. Hypothyroidism
intestinal tract, increased hepatic glucose output, hy- and diabetes has been considered as independent
perinsulinaemia, increased free fatty acid levels and factors for increasing cardiovascular risk. It has been
increased peripheral glucose transport. The most im- well proven that hypothyroidism affects cardiovascu-
portant mechanism seems to be increased hepatic lar dynamics is several ways including increased sys-
glucose output leading to hyperinsulinaemia, further temic vascular resistance, diastolic dysfunction, re-
progression to glucose intolerance and development duced systolic function and reduced cardiac preload.
of peripheral insulin resistance. This development Treatment with appropriate thyroxine dosage revers-
may even proceed to extremes such as ketoacidosis es these abnormalities. The increased cardiovascular
both in type 1 and type 2 diabetes. Severe hyperthy- risk can be attributed to dyslipidaemia predominantly
roidism has significant anti-lipolytic effects and in- increased LDL, diastolic dysfunction, increased arte-
creased β-oxidation of thyrotoxicosis. The increased rial stiffness, altered coagulability and raised hs-CRP.
insulin requirements will subside when thyrotoxicosis These abnormalities are also present in diabetes,
is treated. In patients with unexplained diabetic ke- which aggravates risk. Lipoprotein a is also found
toacidosis, thyrotoxicosis has to be excluded as a to be increased individuals with hypothyroidism and
precipitating factor.
diabetes in independent studies which has been a
Hypothyroidism and diabetes are well known to good surrogate marker of predicting cardiovascular
affect the cardiovascular system in multiple ways. disease. In a large meta-analysis evaluating subclin-
Cardio Diabetes Medicine