
Page 384 - fbkCardioDiabetes_2017
P. 384
360 Cardio Diabetes Medicine 2017
Figure -4.V4R in inferior MI Figure- 6
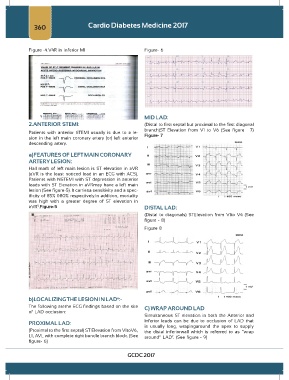
MID LAD:
2.ANTERIOR STEMI: (Distal to first septal but proximal to the first diagonal
branch)ST Elevation from V1 to V6 (See figure – 7)
Patients with anterior STEMI usually is due to a le- Figure- 7
sion in the left main coronary artery (or) left anterior
descending artery.
a)FEATURES OF LEFT MAIN CORONARY
ARTERY LESION:
Hall mark of left main lesion is ST elevation in aVR
(aVR is the least noticed lead in an ECG with ACS).
Patients with NSTEMI with ST depression in anterior
leads with ST Elevation in aVRmay have a left main
lesion (See figure-5). It carriesa sensitivity and a spec-
ificity of 85% &80% respectively.In addition, mortality
was high with a greater degree of ST elevation in
aVR .Figure-5 DISTAL LAD:
5
(Distal to diagonals) STElevation from V1to V4 (See
figure - 8)
Figure 8
b)LOCALIZING THE LESION IN LAD :-
6
The following arethe ECG findings based on the site C) WRAP AROUND LAD
of LAD occlusion:
Simultaneous ST elevation in both the Anterior and
PROXIMAL LAD: Inferior leads can be due to occlusion of LAD that
is usually long, wrapingaround the apex to supply
(Proximal to the first septal) ST Elevation from V1toV6, the distal inferiorwall which is referred to as “wrap
L1, AVL with complete right bundle branch block. (See around” LAD . (See figure - 9)
7
figure- 6)
GCDC 2017