
Page 315 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 315
CHAPTER 30: Interventional Radiology 219
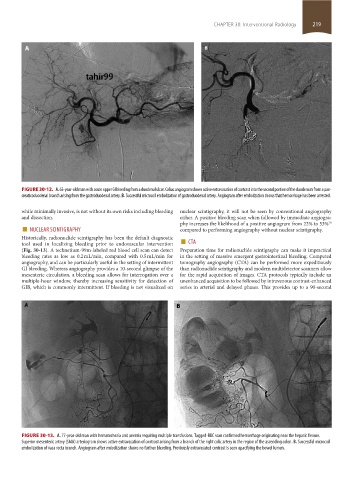
FIGURE 30-12. A. 63-year-old man with acute upper GI bleeding from a duodenal ulcer. Celiac angiogram shows active extravasation of contrast into the second portion of the duodenum from a pan-
creaticoduodenal branch arising from the gastroduodenal artery. B. Successful microcoil embolization of gastroduodenal artery. Angiogram after embolization shows that hemorrhage has been arrested.
while minimally invasive, is not without its own risks including bleeding nuclear scintigraphy, it will not be seen by conventional angiography
and dissection. either. A positive bleeding scan when followed by immediate angiogra-
■ NUCLEAR SCINTIGRAPHY phy increases the likelihood of a positive angiogram from 22% to 53%
30
compared to performing angiography without nuclear scintigraphy.
tool used in localizing bleeding prior to endovascular intervention ■ CTA
Historically, radionuclide scintigraphy has been the default diagnostic
(Fig. 30-13). A technetium-99m-labeled red blood cell scan can detect Preparation time for radionuclide scintigraphy can make it impractical
bleeding rates as low as 0.2 mL/min, compared with 0.5 mL/min for in the setting of massive emergent gastrointestinal bleeding. Computed
angiography, and can be particularly useful in the setting of intermittent tomography angiography (CTA) can be performed more expeditiously
GI bleeding. Whereas angiography provides a 10-second glimpse of the than radionuclide scintigraphy and modern multidetector scanners allow
mesenteric circulation, a bleeding scan allows for interrogation over a for the rapid acquisition of images. CTA protocols typically include an
multiple-hour window, thereby increasing sensitivity for detection of unenhanced acquisition to be followed by intravenous contrast-enhanced
GIB, which is commonly intermittent. If bleeding is not visualized on series in arterial and delayed phases. This provides up to a 90-second
FIGURE 30-13. A. 77-year-old man with hematochezia and anemia requiring multiple transfusions. Tagged-RBC scan confirmed hemorrhage originating near the hepatic flexure.
Superior mesenteric artery (SMA) arteriogram shows active extravasation of contrast arising from a branch of the right colic artery in the region of the ascending colon. B. Successful microcoil
embolization of vasa recta branch. Angiogram after embolization shows no further bleeding. Previously extravasated contrast is seen opacifying the bowel lumen.
section02.indd 219 1/13/2015 2:05:58 PM