
Page 572 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 572
392 PART 4: Pulmonary Disorders
1. Assess the likelihood and clinical impact of basic management problems:
• Difficulty with patient cooperation or consent
• Difficult mask ventilation
• Difficult supraglottic airway placement
• Difficult laryngoscopy
• Difficult intubation
• Difficult surgical airway access
2. Actively pursue opportunities to deliver supplemental oxygen throughout the process of difficult airway
management.
3. Consider the relative merits and feasibility of basic management choices:
• Awake intubation vs intubation after induction of general anesthesia
• Non invasive technique vs invasive techniques for the initial approach to intubation
• Video-assisted laryngoscopy as an initial approach to intubation
• Preservation vs ablation of spontaneous ventilation
4. Develop primary and alternative strategies:
Awake intubation Intubation after
induction of general anesthesia
Airway approached by Invasive airway access (b)*
noninvasive intubation Initial intubation Initial intubation
attempts successful* attempts unsuccessful
From this point onward
Succeed* Fail consider:
1. Calling for help
2. Returning to
Cancel Consider feasibility Invasive
case of other options (a) airway access (b)* spontaneous ventilation
3. Awakening the patient
Face mask ventilation adequate Face mask ventilation not adequate
Consider/attempt SGA
SGA adequate* SGA not adequate
or not feasible
Nonemergency pathway Emergency pathway
ventilation adequate, intubation unsuccessful ventilation not adequate, intubation unsuccessful
If both
Alternative approaches face mask Call for help
and SGA
to intubation (c) ventilation
become Emergency noninvasive airway ventilation (a)
inadequate
Successful Fail after
intubation* multiple attempts Successful ventilation* Fail
Emergency
Invasive Consider feasibility Awaken invasive airway
airway access (b)* of other options (a) patient (d) access (b)*
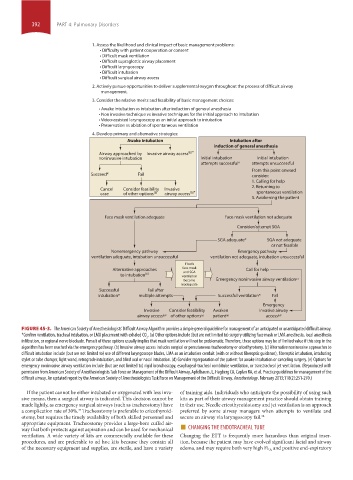
FIGURE 45-3. The American Society of Anesthesiologists’ Difficult Airway Algorithm provides a simple general guideline for management of an anticipated or unanticipated difficult airway.
*Confirm ventilation, tracheal intubation, or LMA placement with exhaled CO . (a) Other options include (but are not limited to) surgery utilizing face mask or LMA anesthesia, local anesthesia
2
infiltration, or regional nerve blockade. Pursuit of these options usually implies that mask ventilation will not be problematic. Therefore, these options may be of limited value if this step in the
algorithm has been reached via the emergency pathway. (b) Invasive airway access includes surgical or percutaneous tracheostomy or cricothyrotomy. (c) Alternative noninvasive approaches to
difficult intubation include (but are not limited to) use of different laryngoscope blades, LMA as an intubation conduit (with or without fiberoptic guidance), fiberoptic intubation, intubating
stylet or tube changer, light wand, retrograde intubation, and blind oral or nasal intubation. (d) Consider repreparation of the patient for awake intubation or canceling surgery. (e) Options for
emergency noninvasive airway ventilation include (but are not limited to) rigid bronchoscopy, esophageal-tracheal combitube ventilation, or transtracheal jet ventilation. (Reproduced with
permission from American Society of Anesthesiologists Task Force on Management of the Difficult Airway, Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice guidelines for management of the
difficult airway. An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. February 2013;118(2):251-270.)
If the patient cannot be either intubated or oxygenated with less inva- of training aids. Individuals who anticipate the possibility of using such
sive means, then a surgical airway is indicated. This decision cannot be kits as part of their airway management practice should obtain training
made lightly, as emergency surgical airways (such as tracheostomy) have in their use. Needle cricothyroidotomy and jet ventilation is an approach
a complication rate of 30%. Tracheostomy is preferable to cricothyroid- preferred by some airway managers when attempts to ventilate and
37
otomy, but requires the timely availability of both skilled personnel and secure an airway via laryngoscopy fail. 38
way that both protects against aspiration and can be used for mechanical ■ CHANGING THE ENDOTRACHEAL TUBE
appropriate equipment. Tracheostomy provides a large-bore cuffed air-
ventilation. A wide variety of kits are commercially available for these Changing the ETT is frequently more hazardous than original inser-
procedures, and are preferable to ad hoc kits because they contain all tion, because the patient may have evolved significant facial and airway
of the necessary equipment and supplies, are sterile, and have a variety edema, and may require both very high Fi O 2 and positive end-expiratory
section04.indd 392 1/23/2015 2:18:55 PM