
Page 631 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 631
450 PART 4: Pulmonary Disorders
100% O 2 The overall goal of this chapter is to provide a comprehensive and
updated clinical approach to ALI and ARDS that is evidence-based
and grounded in current concepts of pathogenesis and pathophysiology.
Objectives include (1) to present the definitions, epidemiology, and
precipitating causes of ALI and ARDS; (2) to describe efforts to predict
the development of ALI and ARDS and to prevent its development;
(3) to describe the pathogenesis and pathophysiology of ALI and ARDS;
(4) to describe the differential diagnosis of ALI and ARDS and clinical
approaches to distinguish among various causes of AHRF; (5) to review
Pa = 650
O 2
the current status of treatment for ALI and ARDS and their precipitating
–
PV = 40 mm Hg causes; (6) to provide current recommendations for ventilatory manage-
O 2
ment of ALI and ARDS; (7) to review so-called “salvage” therapies for
–
CV = 15 mL % refractory ARDS. The last objective includes a detailed description of
O 2
the low-tidal-volume ventilatory strategy used by the ARDS Clinical
Trials Network (ARDSNet) investigators in the clinical trials spon-
C CO 2 = 22 mL % sored by the National Heart, Lung, and Blood Institute (NHLBI) of the
National Institutes of Health (NIH). 3,4
DESCRIPTION AND DEFINITIONS OF ALI AND ARDS
Ca = 18.5 mL % ARDS was initially described in 1967 by Ashbaugh and coauthors as a
O 2
Pa = 60 mm Hg syndrome characterized by the acute onset of dyspnea, severe hypox-
O 2
emia, diffuse lung infiltrates, and decreased compliance of the respira-
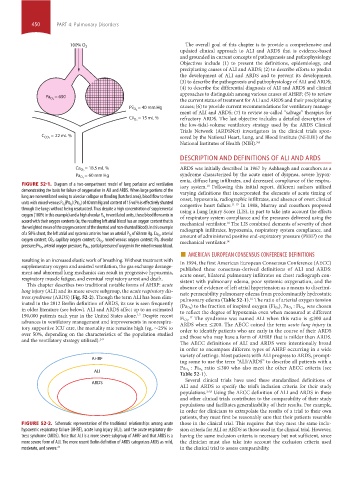
FIGURE 52-1. Diagram of a two-compartment model of lung perfusion and ventilation tory system. Following this initial report, different authors utilized
10
dem onstrating the basis for failure of oxygenation in ALI and ARDS. When large portions of the varying definitions that incorporated the elements of acute timing of
lung are nonventilated owing to alveolar collapse or flooding (hatched area), blood flow to these onset, hypoxemia, radiographic infiltrates, and absence of overt clinical
– – ) of 40 mm Hg and content of 15 vol% is effectively shunted
units with mixed venous P O 2 (Pv O 2 )(Pv O 2 congestive heart failure. 11-15 In 1988, Murray and coauthors proposed
through the lungs without being resaturated. Thus despite a high concentration of supplemental using a Lung Injury Score (LIS), in part to take into account the effects
in ventilated units, these blood flows mix in
oxygen (100% in this example) and a high alveolar P O 2 of respiratory system compliance and the pressures delivered using the
accord with their oxygen contents (ie, the resulting left atrial blood has an oxygen content that is mechanical ventilator. The LIS combined elements of severity of chest
14
the weighted mean of the oxygen content of the shunted and non-shunted blood). In this example radiograph infiltrates, hypoxemia, respiratory system compliance, and
, arterial
of a 50% shunt, the left atrial and systemic arteries have an arterial P O 2 of 60 mm Hg. Ca O 2 amount of administered positive end-expiratory pressure (PEEP) on the
– , mixed venous oxygen content; Pa, alveolar
oxygen content; CO 2, capillary oxygen content; Cv O 2 mechanical ventilator. 14
–
■ AMERICAN EUROPEAN CONSENSUS CONFERENCE DEFINITIONS
pressure; Pv O 2 , arterial oxygen pressure; Pa O 2 , partial pressure of oxygen in the mixed venous blood.
resulting in an increased elastic work of breathing. Without treatment with In 1994, the first American European Consensus Conference (AECC)
supplementary oxygen and assisted ventilation, the gas exchange derange- published these consensus-derived definitions of ALI and ARDS:
ment and abnormal lung mechanics can result in progressive hypoxemia, acute onset, bilateral pulmonary infiltrates on chest radiograph con-
respiratory muscle fatigue, and eventual respiratory arrest and death. sistent with pulmonary edema, poor systemic oxygenation, and the
This chapter describes two traditional notable forms of AHRF: acute absence of evidence of left atrial hypertension as a means to discrimi-
lung injury (ALI) and its more severe subgroup, the acute respiratory dis- nate permeability pulmonary edema from predominantly hydrostatic
tress syndrome (ARDS) (Fig. 52-2). Though the term ALI has been elim- pulmonary edema (Table 52-1). The ratio of arterial oxygen tension
16
inated in the 2012 Berlin definition of ARDS, its use is seen frequently , was chosen
in older literature (see below). ALI and ARDS affect up to an estimated (Pa O 2 ) to the fraction of inspired oxygen (Fi O 2 ), Pa O 2 : Fi O 2
to reflect the degree of hypoxemia even when measured at different
190,000 patients each year in the United States alone. Despite recent . The syndrome was named ALI when this ratio is ≤300 and
1,2
17
advances in ventilatory management and improvements in nonrespira- Fi O 2
ARDS when ≤200. The AECC coined the term acute lung injury in
tory supportive ICU care, the mortality rate remains high (eg, ∼25% to order to identify patients who are early in the course of their ARDS
over 50%, depending on the characteristics of the population studied and those who may have a form of AHRF that is milder than ARDS.
and the ventilatory strategy utilized). 2-9 The AECC definitions of ALI and ARDS were intentionally broad
in order to encompass different types of AHRF occurring in a wide
variety of settings. Most patients with ALI progress to ARDS, prompt-
AHRF
ing some to use the term “ALI/ARDS” to describe all patients with a
ratio ≤300 who also meet the other AECC criteria (see
ALI Pa O 2 : Fi O 2
Table 52-1).
Several clinical trials have used these standardized definitions of
ARDS
ALI and ARDS to specify the trial’s inclusion criteria for their study
populations. 3,4,8 Using the AECC definition of ALI and ARDS in these
and other clinical trials contributes to the comparability of their study
populations and facilitates generalizability of their results. For example,
in order for clinicians to extrapolate the results of a trial to their own
patients, they must first be reasonably sure that their patients resemble
FIGURE 52-2. Schematic representation of the traditional relationships among acute those in the clinical trial. This requires that they meet the same inclu-
hypoxemic respiratory failure (AHRF), acute lung injury (ALI), and the acute respiratory dis- sion criteria for ALI or ARDS as those used in the clinical trial. However,
tress syndrome (ARDS). Note that ALI is a more severe subgroup of AHRF and that ARDS is a having the same inclusion criteria is necessary but not sufficient, since
more severe form of ALI. The more recent Berlin definition of ARDS categorizes ARDS as mild, the clinician must also take into account the exclusion criteria used
moderate, and severe. 24 in the clinical trial to assess comparability.
section04.indd 450 1/23/2015 2:19:33 PM