
Page 281 - Clinical Anatomy
P. 281
ECA5 7/18/06 6:50 PM Page 266
266 The head and neck
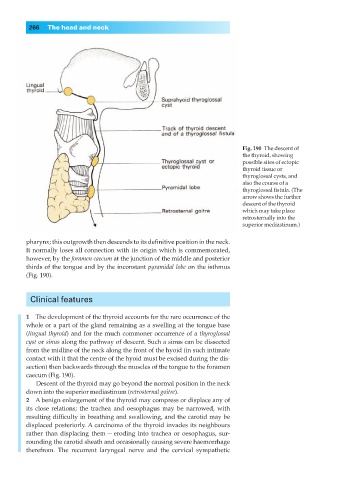
Fig. 190◊The descent of
the thyroid, showing
possible sites of ectopic
thyroid tissue or
thyroglossal cysts, and
also the course of a
thyroglossal fistula. (The
arrow shows the further
descent of the thyroid
which may take place
retrosternally into the
superior mediastinum.)
pharynx; this outgrowth then descends to its definitive position in the neck.
It normally loses all connection with its origin which is commemorated,
however, by the foramen caecum at the junction of the middle and posterior
thirds of the tongue and by the inconstant pyramidal lobe on the isthmus
(Fig. 190).
Clinical features
1◊◊The development of the thyroid accounts for the rare occurrence of the
whole or a part of the gland remaining as a swelling at the tongue base
(lingual thyroid) and for the much commoner occurrence of a thyroglossal
cyst or sinus along the pathway of descent. Such a sinus can be dissected
from the midline of the neck along the front of the hyoid (in such intimate
contact with it that the centre of the hyoid must be excised during the dis-
section) then backwards through the muscles of the tongue to the foramen
caecum (Fig. 190).
Descent of the thyroid may go beyond the normal position in the neck
down into the superior mediastinum (retrosternal goitre).
2◊◊A benign enlargement of the thyroid may compress or displace any of
its close relations; the trachea and oesophagus may be narrowed, with
resulting difficulty in breathing and swallowing, and the carotid may be
displaced posteriorly. A carcinoma of the thyroid invades its neighbours
rather than displacing them — eroding into trachea or oesophagus, sur-
rounding the carotid sheath and occasionally causing severe haemorrhage
therefrom. The recurrent laryngeal nerve and the cervical sympathetic