
Page 329 - Clinical Anatomy
P. 329
ECA5 7/18/06 6:51 PM Page 314
314 The head and neck
The aponeurotic layer is under tension because of its muscular com-
ponent and retracts on the underlying loose layer when divided; a
gaping scalp wound must, therefore, have extended at least through the
aponeurosis.
The periosteum adheres to the suture-lines of the skull; collections of pus
or blood beneath this layer, therefore, outline the affected bone. This is par-
ticularly well seen in birth injuries involving the skull (cephalohaematoma).
The skull (Figs 222, 223, 224)
The important regional anatomy of the skull is dealt with under the appro-
priate headings (ear, nose, accessory sinuses, etc.). Collected together in this
section are some general facts of clinical relevance.
The bony vault of the skull is relatively elastic in consistency; thus a
blow may injure the underlying brain without fracturing bone. Where the
cranium is protected by thick muscle (the lower part of the occipital bone
and the squamous temporal), the skull is correspondingly thin; if held up to
the light it can be seen to be translucent at these sites.
The palpable landmarks of the skull are enumerated in the section on
the surface anatomy of the head (page 311). Radiologically, the sutures
between the vault bones are important because they, as well as the vascular
markings of the meningeal and diploic vessels, may be confused with frac-
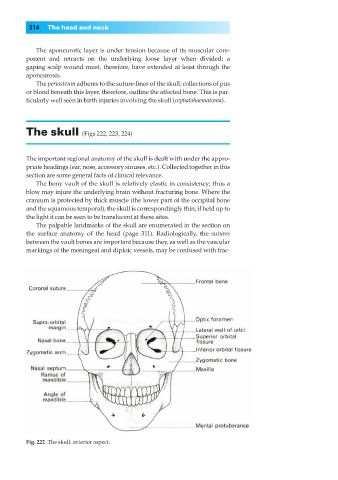
Fig. 222◊The skull: anterior aspect.