
Page 37 - Clinical Anatomy
P. 37
ECA1 7/18/06 6:31 PM Page 22
22 The Thorax
2nd costal
cartilage
Internal
thoracic artery
and veins
Thymus
Superior
vena cava
Right phrenic
nerve Left phrenic
nerve
Azygos vein
Right vagus Left vagus
nerve nerve
Trachea Left recurrent
Oesophagus laryngeal nerve
Aortic arch
T4 Thoracic
duct
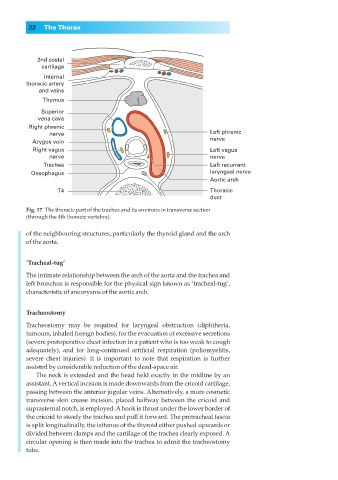
Fig. 17◊The thoracic part of the trachea and its environs in transverse section
(through the 4th thoracic vertebra).
of the neighbouring structures, particularly the thyroid gland and the arch
of the aorta.
‘Tracheal-tug’
The intimate relationship between the arch of the aorta and the trachea and
left bronchus is responsible for the physical sign known as ‘tracheal-tug’,
characteristic of aneurysms of the aortic arch.
Tracheostomy
Tracheostomy may be required for laryngeal obstruction (diphtheria,
tumours, inhaled foreign bodies), for the evacuation of excessive secretions
(severe postoperative chest infection in a patient who is too weak to cough
adequately), and for long-continued artificial respiration (poliomyelitis,
severe chest injuries). It is important to note that respiration is further
assisted by considerable reduction of the dead-space air.
The neck is extended and the head held exactly in the midline by an
assistant. A vertical incision is made downwards from the cricoid cartilage,
passing between the anterior jugular veins. Alternatively, a more cosmetic
transverse skin crease incision, placed halfway between the cricoid and
suprasternal notch, is employed. Ahook is thrust under the lower border of
the cricoid to steady the trachea and pull it forward. The pretracheal fascia
is split longitudinally, the isthmus of the thyroid either pushed upwards or
divided between clamps and the cartilage of the trachea clearly exposed. A
circular opening is then made into the trachea to admit the tracheostomy
tube.