
Page 208 - Cardiac Nursing
P. 208
c.
7-2
p
t
t
03.
q
03.
7-2
c.
ara
e 1
p
84
g
e 1
84
ara
A
p
A
q
6 P
M
6 P
0:1
0:1
g
g
Pa
M
Pa
1
6
6
xd
q
xd
/09
1
/09
/29
/29
In
In
17
08_
p
p
a
a
17
LWB
K34
LWBK340-c08_ pp177-203.qxd 6/29/09 10:16 PM Page 184 Aptara Inc.
LWB
K34
08_
0-c
0-c
184 PA R T I I / Physiologic and Pathologic Responses
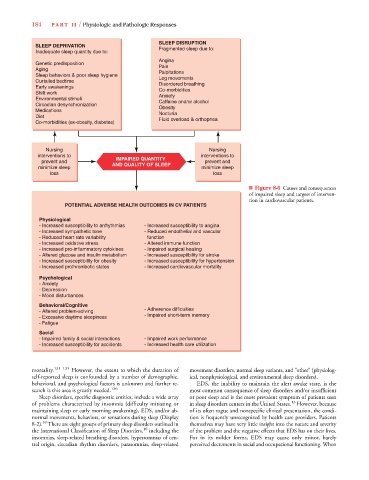
SLEEP DISRUPTION
SLEEP DEPRIVATION Fragmented sleep due to:
Inadequate sleep quantity due to:
Angina
Genetic predisposition Pain
Aging Palpitations
Sleep behaviors & poor sleep hygiene Leg movements
Curtailed bedtime
Early awakenings Disordered breathing
Co-morbidities
Shift work Anxiety
Environmental stimuli Caffeine and/or alcohol
Circadian desynchronization Obesity
Medications
Diet Nocturia
Fluid overload & orthopnea
Co-morbidities (ex-obesity, diabetes)
Nursing Nursing
interventions to interventions to
prevent and IMPAIRED QUANTITY prevent and
minimize sleep AND QUALITY OF SLEEP minimize sleep
loss loss
■ Figure 8-6 Causes and consequences
of impaired sleep and targets of interven-
tion in cardiovascular patients.
POTENTIAL ADVERSE HEALTH OUTCOMES IN CV PATIENTS
Physiological
- Increased susceptibility to arrhythmias - Increased susceptibility to angina
- Increased sympathetic tone - Reduced endothelial and vascular
- Reduced heart rate variability function
- Increased oxidative stress - Altered immune function
- Increased pro-inflammatory cytokines - Impaired surgical healing
- Altered glucose and insulin metabolism - Increased susceptibility for stroke
- Increased susceptibility for obesity - Increased susceptibility for hypertension
- Increased prothrombotic states - Increased cardiovascular mortality
Psychological
- Anxiety
- Depression
- Mood disturbances
Behavioral/Cognitive
- Altered problem-solving - Adherence difficulties
- Excessive daytime sleepiness - Impaired short-term memory
- Fatigue
Social
- Impaired family & social interactions - Impaired work performance
- Increased susceptibility for accidents - Increased health care utilization
mortality. 131–135 However, the extent to which the duration of movement disorders, normal sleep variants, and “other” (physiolog-
self-reported sleep is confounded by a number of demographic, ical, nonphysiological, and environmental sleep disorders).
behavioral, and psychological factors is unknown and further re- EDS, the inability to maintain the alert awake state, is the
search is this area is greatly needed. 136 most common consequence of sleep disorders and/or insufficient
Sleep disorders, specific diagnostic entities, include a wide array or poor sleep and is the most prevalent symptom of patients seen
13
of problems characterized by insomnia (difficulty initiating or in sleep disorders centers in the United States. However, because
maintaining sleep or early morning awakening), EDS, and/or ab- of its often vague and nonspecific clinical presentation, the condi-
normal movements, behaviors, or sensations during sleep (Display tion is frequently unrecognized by health care providers. Patients
10
8-2). There are eight groups of primary sleep disorders outlined in themselves may have very little insight into the nature and severity
the International Classification of Sleep Disorders, 10 including the of the problem and the negative effects that EDS has on their lives.
insomnias, sleep-related breathing disorders, hypersomnias of cen- For in its milder forms, EDS may cause only minor, barely
tral origin, circadian rhythm disorders, parasomnias, sleep-related perceived decrements in social and occupational functioning. When